

Costello syndrome: Analysis of the posterior cranial fossa in children with posterior fossa crowding
- PMID: 26246091
- PMCID: PMC4757298
- DOI: 10.1177/1971400915592549
Costello syndrome: Analysis of the posterior cranial fossa in children with posterior fossa crowding
Abstract
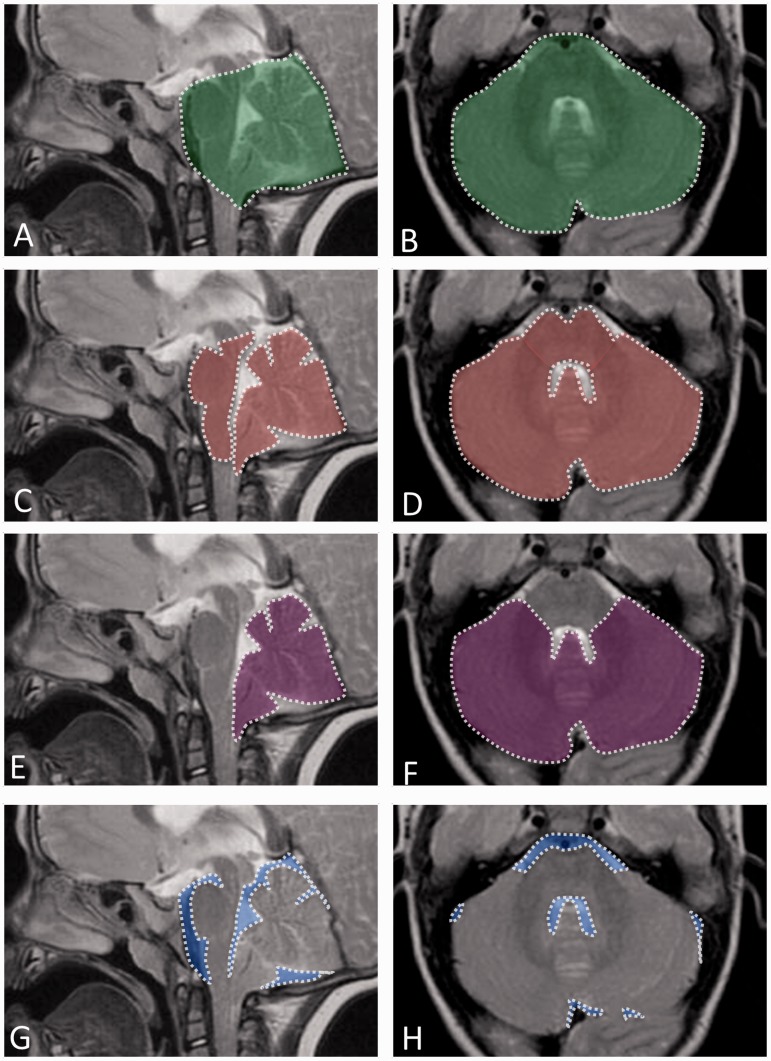
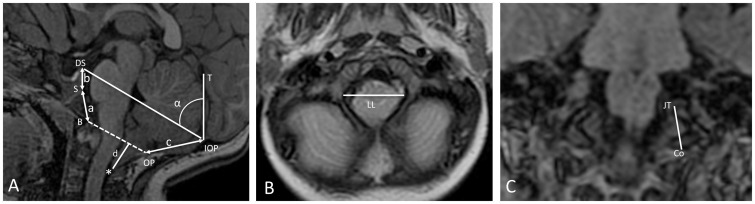
This study aimed to assess changes in the posterior cranial fossa (PCF) to shed light on the mechanism of cerebellar herniation in children with Costello syndrome (CS) and posterior fossa crowding. We performed a morphovolumetric PCF analysis on brain magnetic resonance imaging (MRI) in seven children with CS (mean age 31 ± 16 months) comparing the MRI scans with those of seven age-matched healthy subjects.PCF volume (PCFV), PCF brain volume (PCFBV) and cerebellar volume (CeV) were assessed on axial T2-weighted MRI. Morphometric parameters (diameters of the foramen magnum, tentorial angle, basiocciput, supraocciput, basisphenoid and exocciput lengths) were measured on sagittal T1-weighted MRI. The volume of the cerebrospinal fluid (CSF) spaces was calculated as PCFV minus PCFBV.Five out of seven CS children showed tonsillar herniation in the upper cervical canal; no child had hydrocephalus but three out of seven children showed ventriculomegaly. In addition, the PCFV/PCFBV ratio, PCFV, CSF spaces volume, basiocciput, basisphenoid and exocciput lengths and latero-lateral and antero-posterior diameters of the foramen magnum were significantly reduced, whereas no significant changes were found in supraocciput length, PCFBV, CeV or hindbrain volume. The volumetric reduction of the PCF due to bony posterior fossa hypoplasia is a predisposing factor for developing cerebellar tonsillar herniation through the foramen magnum in children with CS. The altered anatomy of the foramen magnum and upward expansion of the PCF secondary to an increased tentorial slope serves to explain the possible mechanism of cerebellar herniation in patients with CS.
Keywords: Chiari anomaly; Magnetic resonance imaging; posterior cranial fossa.
© The Author(s) 2015.
Figures
References
-
- Lorenz S, Lissewski C, Simsek-Kiper PO, et al. Functional analysis of a duplication (p.E63_D69dup) in the switch II region of HRAS: New aspects of the molecular pathogenesis underlying Costello syndrome. Hum Mol Genet 2013; 22: 1643–1653. - PubMed
-
- Gripp KW, Lin AE, Stabley DL, et al. HRAS mutation analysis in Costello syndrome: Genotype and phenotype correlation. Am J Med Genet A 2006; 140: 1–7. - PubMed
-
- Aoki Y, Niihori T, Kawame H, et al. Germline mutations in HRAS proto-oncogene cause Costello syndrome. Nat Genet 2005; 37: 1038–1040. - PubMed
-
- Rauen KA, Hefner E, Carrillo K, et al. Molecular aspects, clinical aspects and possible treatment modalities for Costello syndrome: Proceedings from the 1st International Costello Syndrome Research Symposium 2007. Am J Med Genet A 2008; 146A: 1205–1217. - PubMed
-
- Rauen KA. HRAS and the Costello syndrome. Clin Genet 2007; 71: 101–108. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
