

Salvage surgery in post-chemoradiation laryngeal and hypopharyngeal carcinoma: outcome and review
- PMID: 26246660
- PMCID: PMC4510934
Salvage surgery in post-chemoradiation laryngeal and hypopharyngeal carcinoma: outcome and review
Abstract
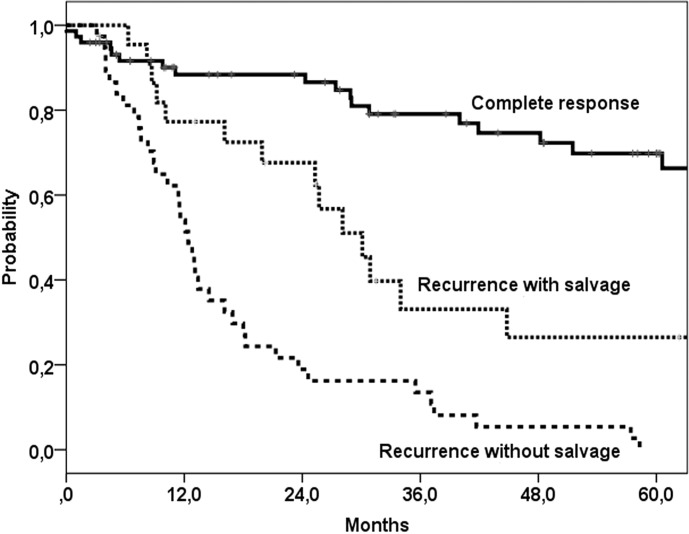
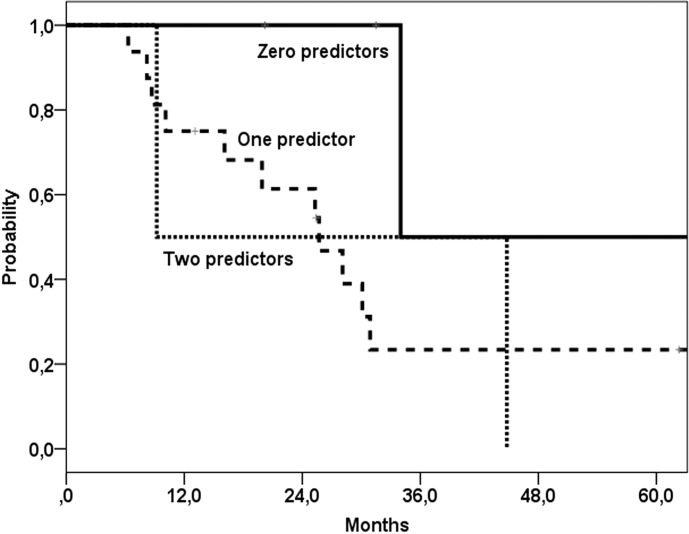
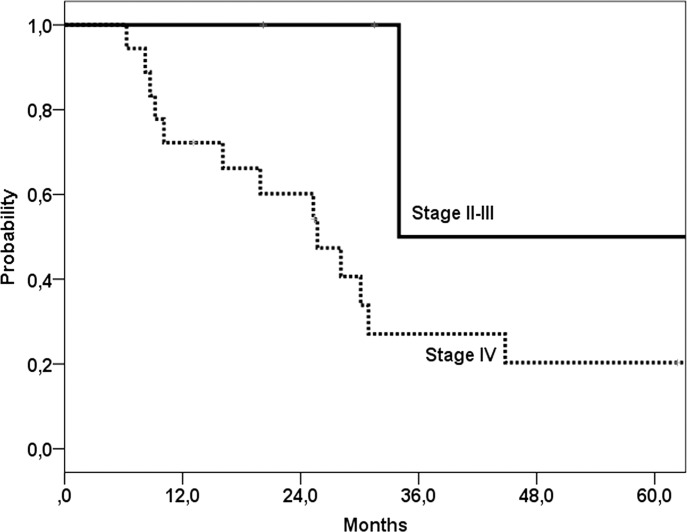
Our objective was to evaluate recurrence patterns of hypopharyngeal and laryngeal carcinoma after chemoradiation and options for salvage surgery, with special emphasis on elderly patients. In a retrospective study all patients who underwent chemoradiation for hypopharyngeal and laryngeal carcinoma in a tertiary care academic center from 1990 through 2010 were evaluated. Primary outcome measures were the survival and complication rates of patients undergoing salvage surgery, especially in elderly patients. Secondary outcome measures were the predictors for salvage surgery for patients with locoregional recurrence after failed chemoradiotherapy. A review of the literature was performed. Of the 136 included patients, 60 patients had recurrent locoregional disease, of whom 22 underwent salvage surgery. Fifteen patients underwent a total laryngectomy with neck dissection(s) and 7 neck dissection without primary tumour surgery. Independent predictors for salvage surgery within the group of 60 patients with recurrent disease, were age under the median of 59 years (p = 0.036) and larynx vs. hypopharynx (p = 0.002) in multivariate analyses. The complication rate was 68% (14% major and 54% minor), with fistulas in 23% of the patients. Significantly more wound related complications occurred in patients with current excessive alcohol use (p = 0.04). Five-year disease free control rate of 35%, overall survival rate of 27% and disease specific survival rate of 35% were found. For the 38 patients who were not suitable for salvage surgery, median survival was 12 months. Patients in whom the tumour was controlled had a 5-year overall survival of 70%. In patients selected for salvage surgery age was not predictive for complications and survival. In conclusion, at two years follow-up after chemoradiation 40% of the patients were diagnosed with recurrent locoregional disease. One third underwent salvage surgery with 35% 5-year disease specific survival and 14% major complications. Older patients selected for salvage surgery had a similar complication rate and survival as younger patients.
Il nostro obiettivo è stato quello di valutare i pattern di recidiva dei carcinomi della laringe e dell'ipofaringe dopo chemioradioterapia, e le opzioni chirurgiche per un trattamento di salvataggio, con particolare attenzione ai pazienti anziani. Sono stati valutati retrospettivamente tutti i pazienti sottoposti a chemioradioterapia per carcinoma dell'ipofaringe e della laringe dal 1990 al 2010, trattati presso un policlinico universitario. Le principali misure dell'outcome sono state la sopravvivenza e il tasso di complicanze dei pazienti sottoposti a chirurgia di salvataggio. Sono stati valutati i fattori predittivi per la chirurgia di salvataggio nei pazienti con recidiva locoregionale dopo fallimento radiochemioterapico. È stata infine eseguita una revisione della letteratura. Dei 136 pazienti inclusi nello studio, 60 hanno avuto una recidiva locoregionale e 22 di questi sono stati sottoposti a chirurgia di salvataggio. 15 pazienti sono stati sottoposti a una laringectomia totale con svuotamento e 7 pazienti sono stati sottoposti solo a svuotamento laterocervicale. Nel gruppo dei 60 pazienti con recidiva di malattia, i fattori predittivi per la chirurgia di salvataggio emersi all'analisi multivariata sono stati l'età inferiore a 59 anni (p = 0,036) e la localizzazione laringea rispetto a quella ipofaringea (p = 0,002). La percentuale di complicanze registrata è stata del 68% (14% maggiori e 54% minori), con il 23% di fistole. Nei pazienti soggetti ad abuso di sostanze alcoliche si è registrata una maggiore quantità di complicanze relative alla ferita chirurgica (p = 0,04). Il controllo di malattia a 5 anni è stato del 35%, la sopravvivenza è stata del 27% e la sopravvivenza cancro specifica è stata del 35%. La sopravvivenza mediana per i 38 pazienti non sottoponibili a chirurgia di salvataggio è stata di 12 mesi. Per i pazienti nei quali si è ottenuto un controllo di malattia la sopravvivenza a 5 anni è stata del 70%. Per i pazienti sottoposti a chirurgia di salvataggio l'età non ha rappresentato un fattore predittivo né della sopravvivenza né del tasso di complicanze. In conclusione dopo due anni di followup dalla chemioradioterapia è stata diagnosticata una recidiva locoregionale nel 40% dei pazienti. Un terzo è stato sottoposto a chirurgia di salvataggio con una sopravvivenza cancro specifica a 5 anni del 35% e un 14% di complicanze maggiori. I pazienti anziani, selezionati per la chirurgia di salvataggio, hanno avuto un tasso di sopravvivenza e di complicanze maggiori sovrapponibili a quelli dei pazienti più giovani.
Keywords: Chemoradiation; Complications; Elderly; Hypopharyngeal cancer; Laryngeal cancer; Review; Salvage surgery; Survival.
Figures
References
-
- Forastiere AA, Goepfert H, Maor M, et al. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N Engl J Med. 2003;349:2091–2098. - PubMed
-
- Wolf GT, Hong WK. Induction chemotherapy for organ preservation in advanced laryngeal cancer: is there a role? Head Neck. 1995;17:279–283. - PubMed
-
- Lefebvre JL, Chevalier D, Luboinski B, et al. Larynx preservation in pyriform sinus cancer: preliminary results of a European Organization for Research and Treatment of Cancer phase III trial. EORTC Head and Neck Cancer Cooperative Group. J Natl Cancer Inst. 1996;88:890–899. - PubMed
-
- Gil Z, Gupta A, Kummer B, et al. The role of pectoralis major muscle flap in salvage total laryngectomy. Arch Otolaryngol Head Neck Surg. 2009;135:1019–1023. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources