

doi: 10.2337/diaclin.32.1.4.
SGLT-2 Inhibitors: A New Mechanism for Glycemic Control
- PMID: 26246672
- PMCID: PMC4521423
- DOI: 10.2337/diaclin.32.1.4
Item in Clipboard
SGLT-2 Inhibitors: A New Mechanism for Glycemic Control
Clin Diabetes.
2014 Jan.
Abstract
Glucosuria, the presence of glucose in the urine, has long been regarded as a consequence of uncontrolled diabetes. However, glucose excretion can be induced by blocking the activity of the renal sodium-glucose cotransporter 2 (SGLT-2). This mechanism corrects hyperglycemia independently of insulin. This article provides an overview of the paradigm shift that triggered the development of the SGLT-2 inhibitor class of agents and summarizes the available evidence from clinical studies to date.
Figures
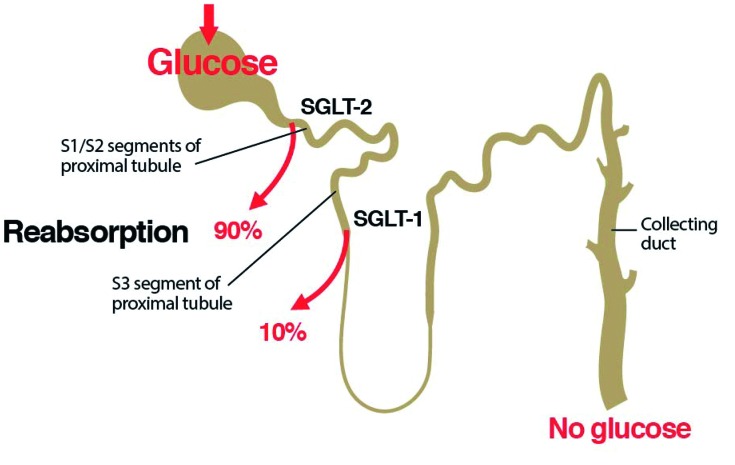
Renal glucose handling. In healthy individuals, the vast majority of the glucose filtered by the kidney is reabsorbed by SGLT-2 in the S1 and S2 segments of the proximal convoluted tubule, and the remaining glucose is reabsorbed by SGLT-1 in the S3 segment.
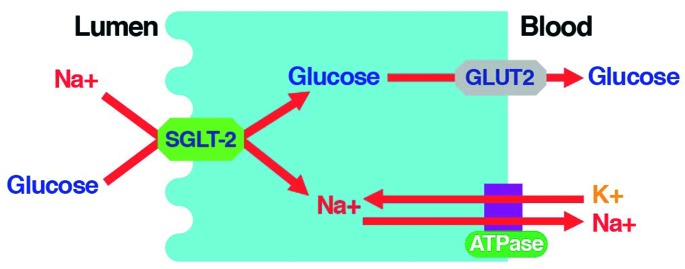
SGLT-2 mediates glucose reabsorption in the kidney. SGLT-2 catalyzes the active transport of glucose (against a concentration gradient) across the luminal membrane by coupling it with the downhill transport of Na+. The inward Na+ gradient across the luminal epithelium is maintained by active extrusion of Na+ across the basolateral surface into the intracellular fluid. Glucose diffuses out of the cell down a concentration gradient via the basolateral facilitative transporter GLUT2. Adapted from Ref. 20.
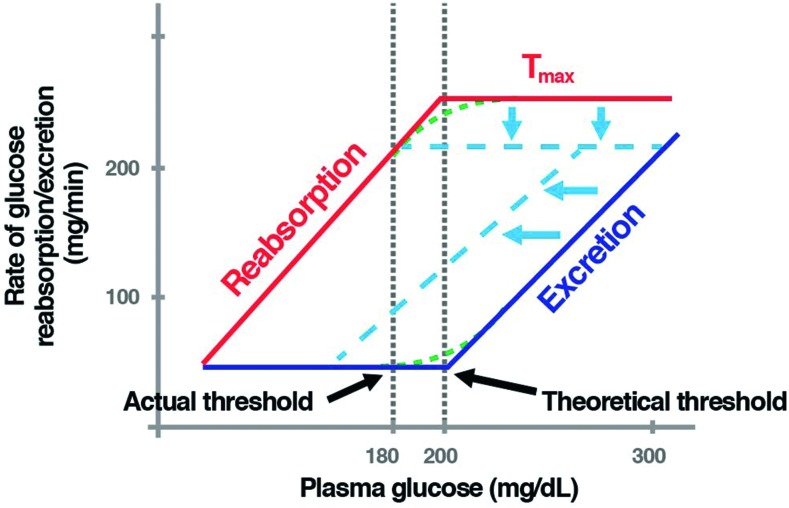
Renal glucose handling before and following inhibition of SGLT-2. As the plasma glucose concentration increases, renal glucose reabsorption increases, following the line marked “Reabsorption” (in red). At plasma glucose concentrations greater than ∼ 200 mg/dl, all the filtered glucose is reabsorbed, and there is no excretion. When glucose reaches a threshold, at ∼ 200 mg/dl, the maximum capacity of the renal tubule to reabsorb glucose—or Tmax—is exceeded. Once past this threshold, glucose begins to be excreted via the urine (dark blue line, labeled “Excretion”). The actual thresholds for both reabsorption and excretion differ from the theoretical thresholds because of physiological variation among individual nephrons (i.e., slight differences in their glucose-handling abilities). This is known as “splay” (green dashed lines). The dashed light blue lines depict renal glucose handling after SGLT-2 inhibition. SGLT-2 inhibitors lower the renal glucose threshold, leading to urinary glucose excretion. Adapted from Ref. 16.
References
-
- Kaiser N, Leibowitz G, Nesher R: Glucotoxicity and beta-cell failure in type 2 diabetes mellitus. J Pediatr Endocrinol Metab 16:5–22, 2003 - PubMed
-
- Centers for Disease Control and Prevention : National diabetes fact sheet: national estimates and general information on diabetes and prediabetes in the United States, 2011. Atlanta, Ga., U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, 2011 Available from http://www.cdc.gov/diabetes/pubs/factsheet11.htm. Accessed 13 August 2013
-
- Centers for Disease Control and Prevention : Press release: Number of Americans with diabetes projected to double or triple by 2050. Older, more diverse population and longer lifespans contribute to increase. 22 October 2010. Available from http://www.cdc.gov/media/pressrel/2010/r101022.html. Accessed 13 August 2013
-
- International Diabetes Federation : IDF Diabetes Atlas. 5th ed. Brussels, Belgium, International Diabetes Federation, 2011 Available from http://www.idforg/diabetesatlas. Accessed 13 August 2013
LinkOut - more resources
Full Text Sources
Other Literature Sources
