

Novel Agents for the Treatment of Type 2 Diabetes
- PMID: 26246766
- PMCID: PMC4522879
- DOI: 10.2337/diaspect.27.2.100
Novel Agents for the Treatment of Type 2 Diabetes
Abstract
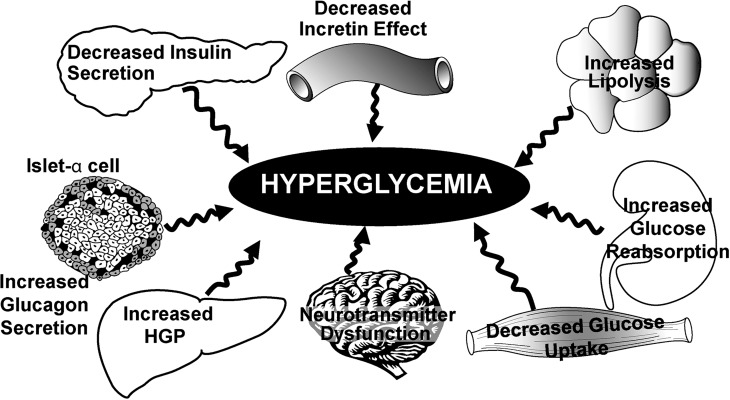
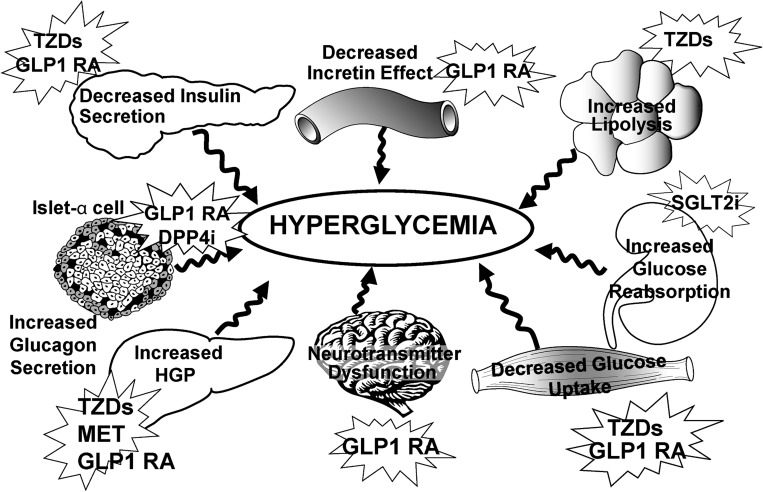
In Brief Impaired insulin secretion, increased hepatic glucose production, and decreased peripheral glucose utilization are the core defects responsible for the development and progression of type 2 diabetes. However, the pathophysiology of this disease also includes adipocyte insulin resistance (increased lipolysis), reduced incretin secretion/sensitivity, increased glucagon secretion, enhanced renal glucose reabsorption, and brain insulin resistance/neurotransmitter dysfunction. Although current diabetes management focuses on lowering blood glucose, the goal of therapy should be to delay disease progression and eventual treatment failure. Recent innovative treatment approaches target the multiple pathophysiological defects present in type 2 diabetes. Optimal management should include early initiation of combination therapy using multiple drugs with different mechanisms of action. This review examines novel therapeutic options that hold particular promise.
Figures
References
-
- DeFronzo RA: Lilly Lecture: the triumvirate: beta cell, muscle, liver: a collusion responsible for NIDDM. Diabetes 37:667–687, 1988 - PubMed
-
- Ferrannini E, Gastaldelli A, Miyazaki Y, Matsuda M, Mari A, DeFronzo RA: Beta cell function in subjects spanning the range from normal glucose tolerance to overt diabetes mellitus: a new analysis. J Clin Endocrinol Metab 90:493–500, 2005 - PubMed
-
- Abdul-Ghani M, Jenkinson C, Richardson D, Tripathy D, DeFronzo RA: Insulin secretion and insulin action in subjects with impaired fasting glucose and impaired glucose tolerance: results from the Veterans Administration Genetic Epidemiology Study (VAGES). Diabetes 55:1430–1435, 2006 - PubMed
-
- Gastaldelli A, Ferrannini E, Miyazaki Y, Matsuda M, DeFronzo RA: Beta cell dysfunction and glucose intolerance: results from the San Antonio Metabolism (SAM) study. Diabetologia 47:31–39, 2004 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
