

Mortality and Financial Burden of Periprosthetic Fractures of the Femur
- PMID: 26246936
- PMCID: PMC4252153
- DOI: 10.1177/2151458514542281
Mortality and Financial Burden of Periprosthetic Fractures of the Femur
Abstract
Objective: This study examines patient factors to identify risks of 12-month mortality following periprosthetic femur fractures. Hospital charges were analyzed to quantify the financial burden for treatment modalities.
Methods: Data were retrospectively analyzed from a prospective database at a university hospital setting. One-hundred and thirteen patients with a periprosthetic fracture of the proximal or distal femur were identified. Risk factors for 12-month mortality were analyzed, and financial data were compared between the various treatment modalities.
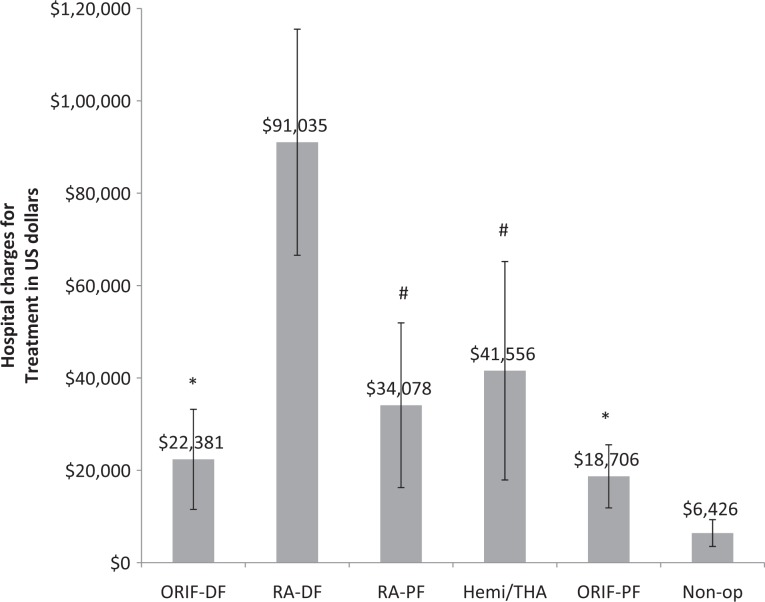
Results: In all, 14% of patients died (16 of 113) within 3 months and the 1-year mortality was 17.7% (20 of 113). Patients who died within 1 year had higher hospital charges (US$33 880 ± 25 051 vs US$22 886 ± 16 841; P = .01) and were older (87.6 ± 8.5 vs 81.5 ± 8.6; P = .004). Logistic regression analysis revealed age was the only significant predictor of 1-year mortality (P = .029, odds ratio 1.1). Analysis of financial data revealed 4 distinct groups (P < .05 between groups). Distal femoral revision arthroplasty (RA-DF) generated the highest hospital charges of US$91 035 ± 25 579 (n = 3). The second most highly charged group included proximal femoral fractures treated with revision arthroplasty (US$34 078 ± 17 832; n = 20) and hemi/total hip arthroplasty (THA; US$41 556 ± 23 651; n = 8). The third most charged group underwent open reduction internal fixation of the proximal (US$18 706 ± 6829; n = 35) and distal (US$22 381 ± 10 835; n = 35) femur. Nonoperative treatment generated the lowest charges (US$6426 ± 2899; n = 11). On average, the hospital lost money treating patients with RA-DF (US$-19 080 ± 2022 per patient) and hemi/THA (US$-6594 ± 9305 per patient), while all other treatment groups were profitable.
Conclusion: One-year mortality after periprosthetic femur fractures was 17.7%, is mostly influenced by age, and 80% of deaths occur within 3 months. Patients treated with primary/revision arthroplasty generate more hospital charges than internal fixation. The average patient treated with revision arthroplasty of the distal femur or hemi/THA for a periprosthetic femur fractures resulted in net financial losses for the hospital.
Keywords: geriatric fracture; hospital charges; mortality; periprosthetic femur fracture.
Conflict of interest statement
Figures
Comment in
-
Substantially higher prevalence of postoperative peri-prosthetic fractures in octogenarians with hip fractures operated with a cemented, polished tapered stem rather than an anatomic stem.Acta Orthop. 2016 Jun;87(3):257-61. doi: 10.3109/17453674.2016.1162898. Epub 2016 Apr 4. Acta Orthop. 2016. PMID: 27045318 Free PMC article.
References
-
- Noor S, Pridham C, Fawcett T, et al. Finite element analysis modelling of proximal femoral fractures, including post-fixation periprosthetic fractures. Injury. 2013;44 (6):791–795. - PubMed
-
- Meek RM, Norwood T, Smith R, Brenkel IJ, Howie CR. The risk of peri-prosthetic fracture after primary and revision total hip and knee replacement. J Bone Joint Surg Br. 2011;93 (1):96–101. - PubMed
-
- Lindahl H. Epidemiology of periprosthetic femur fracture around a total hip arthroplasty. Injury. 2007;38 ( 6 ):651–654. - PubMed
-
- Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89 (4):780–785. - PubMed
-
- Berry DJ. Epidemiology: hip and knee. Orthop Clin North Am. 1999;30 ( 2 ):183–190. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
