

Vital Signs: Estimated Effects of a Coordinated Approach for Action to Reduce Antibiotic-Resistant Infections in Health Care Facilities - United States
- PMID: 26247436
- PMCID: PMC4654955
Vital Signs: Estimated Effects of a Coordinated Approach for Action to Reduce Antibiotic-Resistant Infections in Health Care Facilities - United States
Abstract
Background: Treatments for health care-associated infections (HAIs) caused by antibiotic-resistant bacteria and Clostridium difficile are limited, and some patients have developed untreatable infections. Evidence-supported interventions are available, but coordinated approaches to interrupt the spread of HAIs could have a greater impact on reversing the increasing incidence of these infections than independent facility-based program efforts.
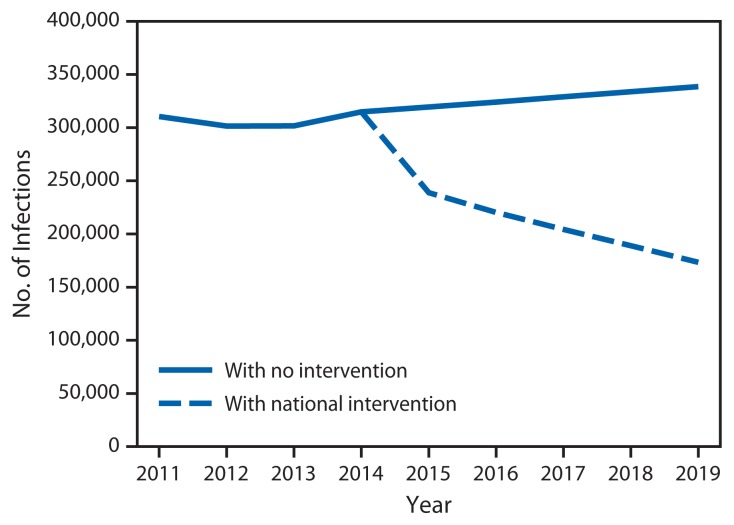
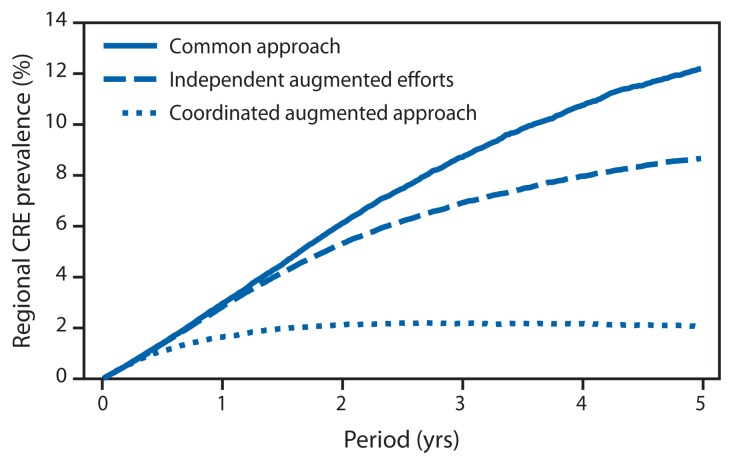
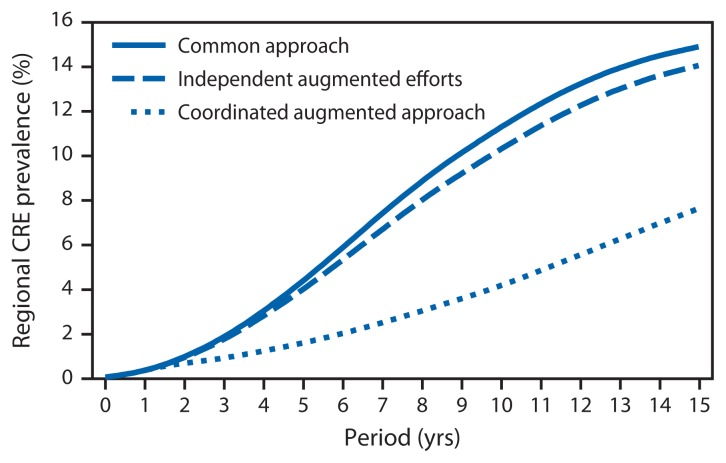
Methods: Data from CDC's National Healthcare Safety Network and Emerging Infections Program were analyzed to project the number of health care-associated infections from antibiotic-resistant bacteria or C. difficile both with and without a large scale national intervention that would include interrupting transmission and improved antibiotic stewardship. As an example, the impact of reducing transmission of one antibiotic-resistant infection (carbapenem-resistant Enterobacteriaceae [CRE]) on cumulative prevalence and number of HAI transmission events within interconnected groups of health care facilities was modeled using two distinct approaches, a large scale and a smaller scale health care network.
Results: Immediate nationwide infection control and antibiotic stewardship interventions, over 5 years, could avert an estimated 619,000 HAIs resulting from CRE, multidrug-resistant Pseudomonas aeruginosa, invasive methicillin-resistant Staphylococcus aureus (MRSA), or C. difficile. Compared with independent efforts, a coordinated response to prevent CRE spread across a group of inter-connected health care facilities resulted in a cumulative 74% reduction in acquisitions over 5 years in a 10-facility network model, and 55% reduction over 15 years in a 102-facility network model.
Conclusions: With effective action now, more than half a million antibiotic-resistant health care-associated infections could be prevented over 5 years. Models representing both large and small groups of interconnected health care facilities illustrate that a coordinated approach to interrupting transmission is more effective than historical independent facilitybased efforts.
Implications for public health: Public health-led coordinated prevention approaches have the potential to more completely address the emergence and dissemination of these antibiotic-resistant organisms and C. difficile than independent facility-based efforts.
Figures
References
-
- CDC. Antibiotic resistance threats in the United States, 2013. Atlanta, GA: US Department of Health and Human Services, CDC; 2013. Available at http://www.cdc.gov/drugresistance/threat-report-2013.
-
- Burton DC, Edwards JR, Horan TC, Jernigan JA, Fridkin SK. Methicillin-resistant Staphylococcus aureus central line-associated bloodstream infections in US intensive care units, 1997–2007. JAMA. 2009;301:727–36. - PubMed
