

Heart Rate Variability Analysis in an Experimental Model of Hemorrhagic Shock and Resuscitation in Pigs
- PMID: 26247476
- PMCID: PMC4527725
- DOI: 10.1371/journal.pone.0134387
Heart Rate Variability Analysis in an Experimental Model of Hemorrhagic Shock and Resuscitation in Pigs
Abstract
Background: The analysis of heart rate variability (HRV) has been shown as a promising non-invasive technique for assessing the cardiac autonomic modulation in trauma. The aim of this study was to evaluate HRV during hemorrhagic shock and fluid resuscitation, comparing to traditional hemodynamic and metabolic parameters.
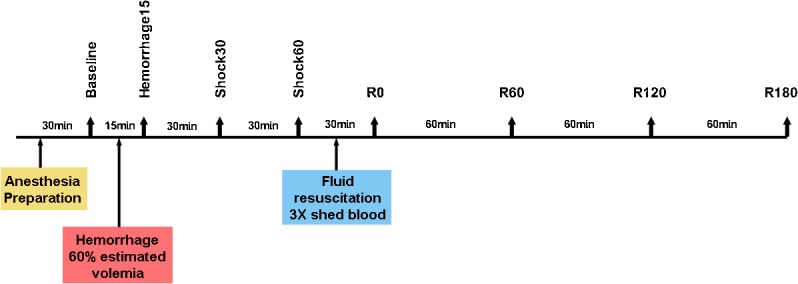
Methods: Twenty anesthetized and mechanically ventilated pigs were submitted to hemorrhagic shock (60% of estimated blood volume) and evaluated for 60 minutes without fluid replacement. Surviving animals were treated with Ringer solution and evaluated for an additional period of 180 minutes. HRV metrics (time and frequency domain) as well as hemodynamic and metabolic parameters were evaluated in survivors and non-survivors animals.
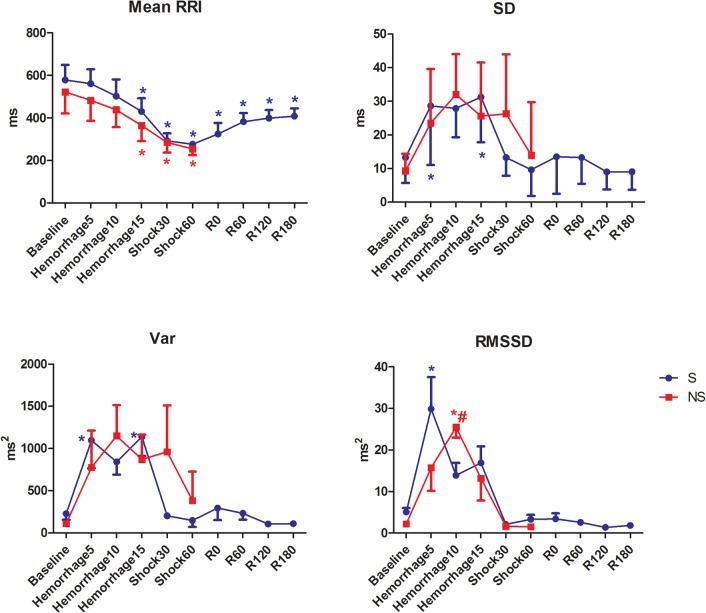
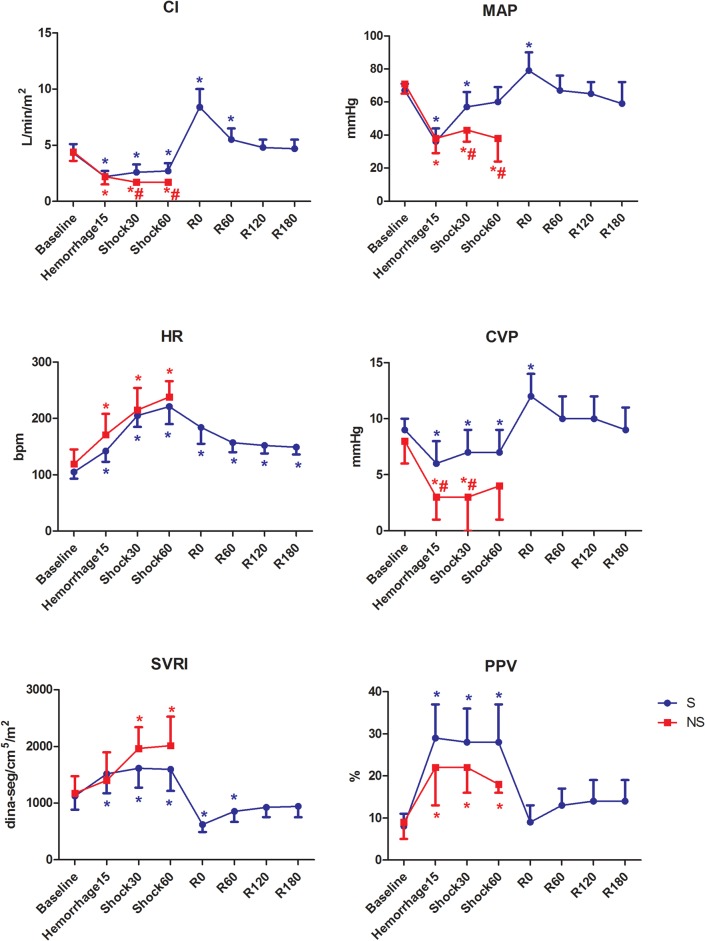
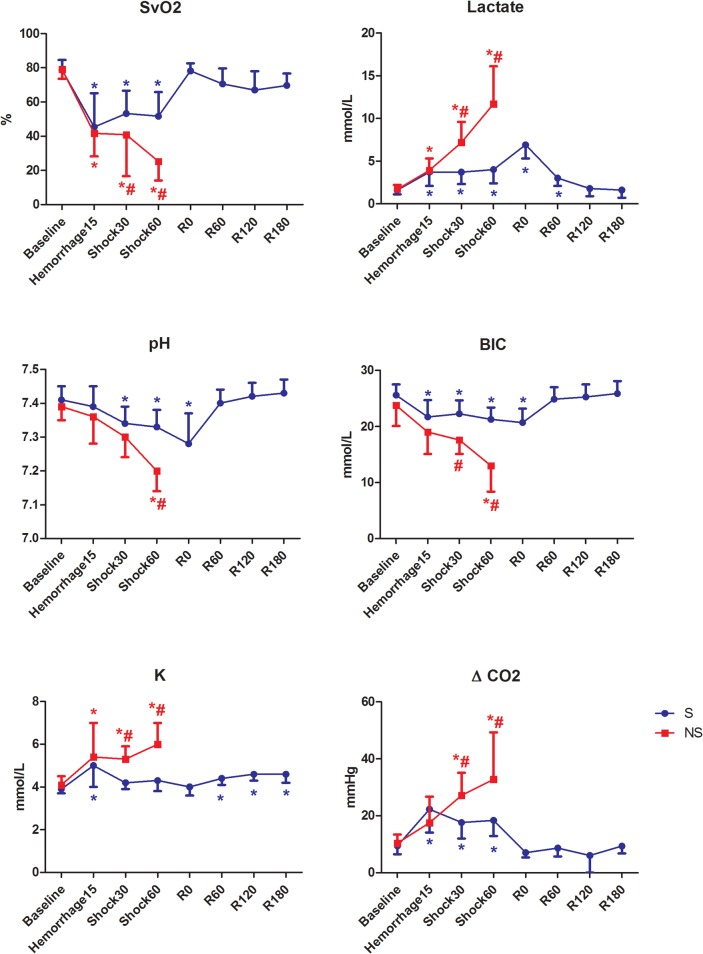
Results: Seven of the 20 animals died during hemorrhage and initial fluid resuscitation. All animals presented an increase in time-domain HRV measures during haemorrhage and fluid resuscitation restored baseline values. Although not significantly, normalized low-frequency and LF/HF ratio decreased during early stages of haemorrhage, recovering baseline values later during hemorrhagic shock, and increased after fluid resuscitation. Non-surviving animals presented significantly lower mean arterial pressure (43±7 vs 57±9 mmHg, P<0.05) and cardiac index (1.7±0.2 vs 2.6±0.5 L/min/m2, P<0.05), and higher levels of plasma lactate (7.2±2.4 vs 3.7±1.4 mmol/L, P<0.05), base excess (-6.8±3.3 vs -2.3±2.8 mmol/L, P<0.05) and potassium (5.3±0.6 vs 4.2±0.3 mmol/L, P<0.05) at 30 minutes after hemorrhagic shock compared with surviving animals.
Conclusions: The HRV increased early during hemorrhage but none of the evaluated HRV metrics was able to discriminate survivors from non-survivors during hemorrhagic shock. Moreover, metabolic and hemodynamic variables were more reliable to reflect hemorrhagic shock severity than HRV metrics.
Conflict of interest statement
Figures
References
-
- Tisherman SA, Schmicker RH, Brasel KJ, Bulger EM, Kerby JD, Minei JP, et al. Detailed description of all deaths in both the shock and traumatic brain injury hypertonic saline trials of the Resuscitation Outcomes Consortium. Annals of surgery. 2015;261(3):586–90. Epub 2014/07/30. 10.1097/SLA.0000000000000837 - DOI - PMC - PubMed
-
- Holcomb JB, Tilley BC, Baraniuk S, Fox EE, Wade CE, Podbielski JM, et al. Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma: the PROPPR randomized clinical trial. JAMA: the journal of the American Medical Association. 2015;313(5):471–82. Epub 2015/02/04. 10.1001/jama.2015.12 . - DOI - PMC - PubMed
-
- Wilson M, Davis DP, Coimbra R. Diagnosis and monitoring of hemorrhagic shock during the initial resuscitation of multiple trauma patients: a review. The Journal of emergency medicine. 2003;24(4):413–22. Epub 2003/05/15. . - PubMed
-
- Cooke WH, Salinas J, Convertino VA, Ludwig DA, Hinds D, Duke JH, et al. Heart rate variability and its association with mortality in prehospital trauma patients. The Journal of trauma. 2006;60(2):363–70; discussion 70. . - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
