

What limits performance during whole-body incremental exercise to exhaustion in humans?
- PMID: 26250346
- PMCID: PMC4606539
- DOI: 10.1113/JP270487
What limits performance during whole-body incremental exercise to exhaustion in humans?
Abstract
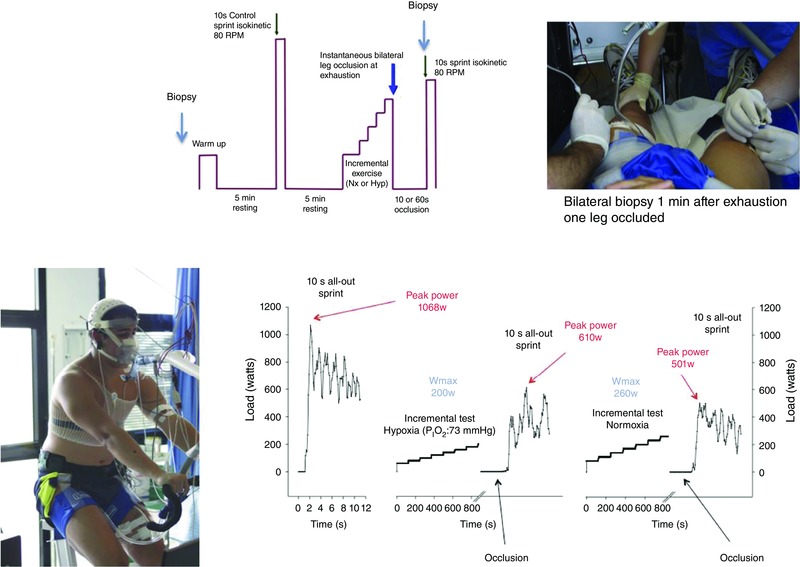
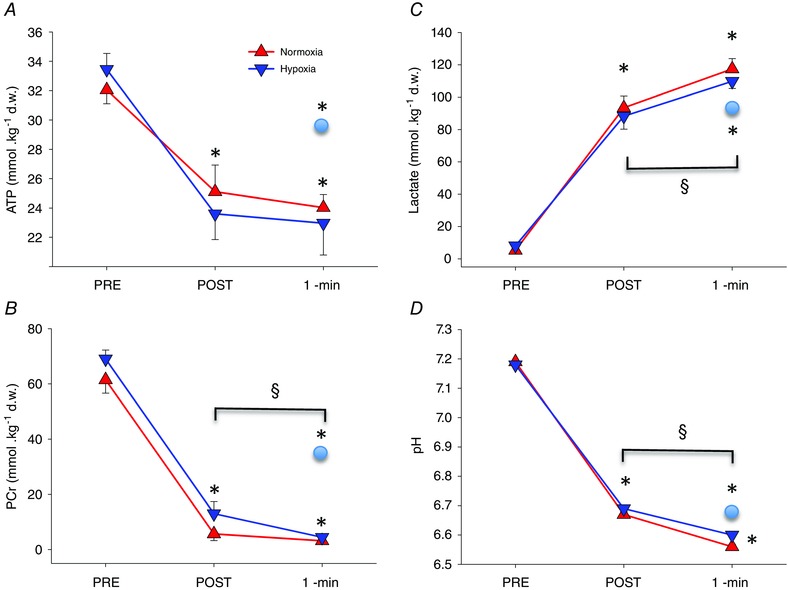
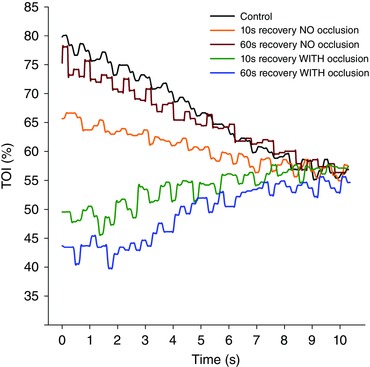
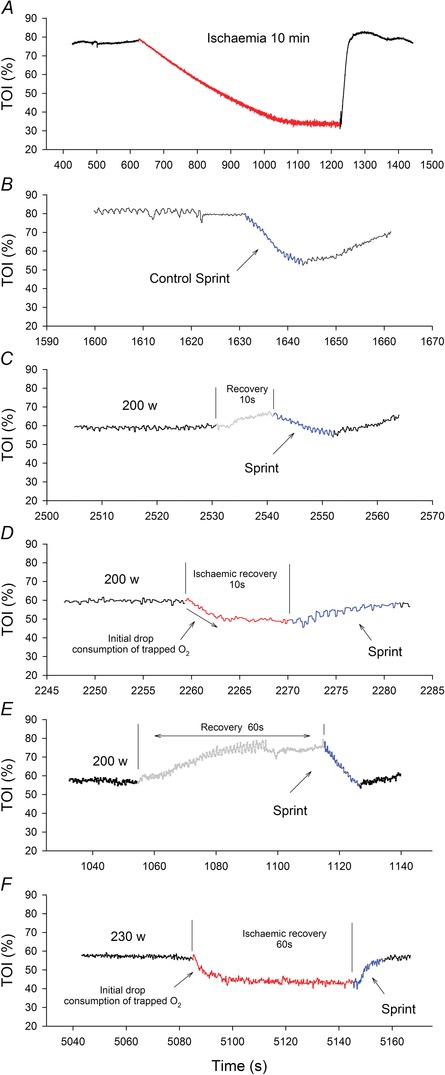
To determine the mechanisms causing task failure during incremental exercise to exhaustion (IE), sprint performance (10 s all-out isokinetic) and muscle metabolites were measured before (control) and immediately after IE in normoxia (P(IO2) 143 mmHg) and hypoxia (P(IO2): 73 mmHg) in 22 men (22 ± 3 years). After IE, subjects recovered for either 10 or 60 s, with open circulation or bilateral leg occlusion (300 mmHg) in random order. This was followed by a 10 s sprint with open circulation. Post-IE peak power output (W(peak)) was higher than the power output reached at exhaustion during IE (P < 0.05). After 10 and 60 s recovery in normoxia, W(peak) was reduced by 38 ± 9 and 22 ± 10% without occlusion, and 61 ± 8 and 47 ± 10% with occlusion (P < 0.05). Following 10 s occlusion, W(peak) was 20% higher in hypoxia than normoxia (P < 0.05), despite similar muscle lactate accumulation ([La]) and phosphocreatine and ATP reduction. Sprint performance and anaerobic ATP resynthesis were greater after 60 s compared with 10 s occlusions, despite the higher [La] and [H(+)] after 60 s compared with 10 s occlusion recovery (P < 0.05). The mean rate of ATP turnover during the 60 s occlusion was 0.180 ± 0.133 mmol (kg wet wt)(-1) s(-1), i.e. equivalent to 32% of leg peak O2 uptake (the energy expended by the ion pumps). A greater degree of recovery is achieved, however, without occlusion. In conclusion, during incremental exercise task failure is not due to metabolite accumulation or lack of energy resources. Anaerobic metabolism, despite the accumulation of lactate and H(+), facilitates early recovery even in anoxia. This points to central mechanisms as the principal determinants of task failure both in normoxia and hypoxia, with lower peripheral contribution in hypoxia.
© 2015 The Authors. The Journal of Physiology © 2015 The Physiological Society.
Figures
References
-
- Allen D & Westerblad H (2004). Physiology. Lactic acid–the latest performance‐enhancing drug. Science 305, 1112–1113. - PubMed
-
- Allen DG, Lamb GD & Westerblad H (2008). Skeletal muscle fatigue: cellular mechanisms. Physiol Rev 88, 287–332. - PubMed
-
- Amann M & Calbet JA (2008). Convective oxygen transport and fatigue. J Appl Physiol (1985) 104, 861–870. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical