

Cytogenetics and long-term survival of patients with refractory or relapsed and refractory multiple myeloma treated with pomalidomide and low-dose dexamethasone
- PMID: 26250580
- PMCID: PMC4591765
- DOI: 10.3324/haematol.2014.117077
Cytogenetics and long-term survival of patients with refractory or relapsed and refractory multiple myeloma treated with pomalidomide and low-dose dexamethasone
Abstract
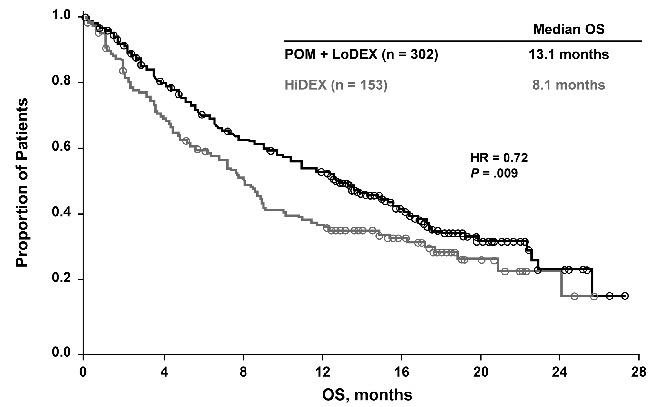
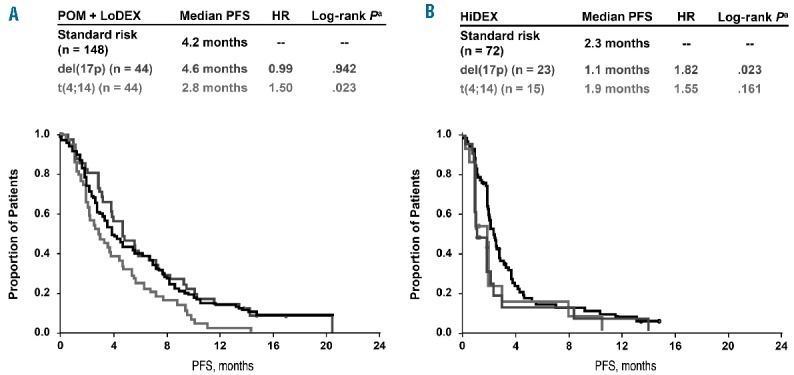
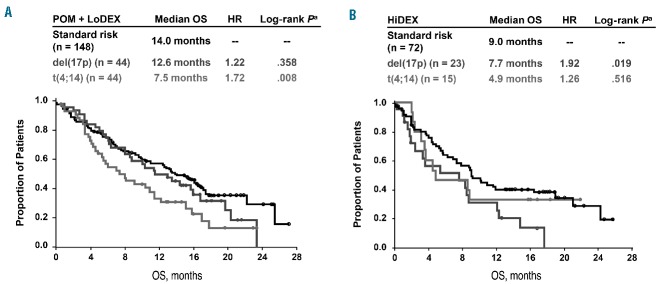
Patients with refractory or relapsed and refractory multiple myeloma who no longer receive benefit from novel agents have limited treatment options and short expected survival. del(17p) and t(4;14) are correlated with shortened survival. The phase 3 MM-003 trial demonstrated significant progression-free and overall survival benefits from treatment with pomalidomide plus low-dose dexamethasone compared to high-dose dexamethasone among patients in whom bortezomib and lenalidomide treatment had failed. At an updated median follow-up of 15.4 months, the progression-free survival was 4.0 versus 1.9 months (HR, 0.50; P<0.001), and median overall survival was 13.1 versus 8.1 months (HR, 0.72; P=0.009). Pomalidomide plus low-dose dexamethasone, compared with high-dose dexamethasone, improved progression-free survival in patients with del(17p) (4.6 versus 1.1 months; HR, 0.34; P <0.001), t(4;14) (2.8 versus 1.9 months; HR, 0.49; P=0.028), and in standard-risk patients (4.2 versus 2.3 months; HR, 0.55; P<0.001). Although the majority of patients treated with high-dose dexamethasone took pomalidomide after discontinuation, the overall survival of patients treated with pomalidomide plus low-dose dexamethasone or high-dose dexamethasone was 12.6 versus 7.7 months (HR, 0.45; P=0.008) in patients with del(17p), 7.5 versus 4.9 months (HR, 1.12; P=0.761) in those with t(4;14), and 14.0 versus 9.0 months (HR, 0.85; P=0.380) in standard-risk subjects. The overall response rate was higher in patients treated with pomalidomide plus low-dose dexamethasone than in those treated with high-dose dexamethasone both among standard-risk patients (35.2% versus 9.7%) and those with del(17p) (31.8% versus 4.3%), whereas it was similar in patients with t(4;14) (15.9% versus 13.3%). The safety of pomalidomide plus low-dose dexamethasone was consistent with initial reports. In conclusion, pomalidomide plus low-dose dexamethasone is efficacious in patients with relapsed/refractory multiple myeloma and del(17p) and/or t(4;14). This study is registered at ClinicalTrials.gov as NCT01311687 and with EudraCT as 2010-019820-30.
Copyright© Ferrata Storti Foundation.
Figures
References
-
- Avet-Loiseau H, Attal M, Moreau P, et al. Genetic abnormalities and survival in multiple myeloma: the experience of the Intergroupe Francophone du Myélome. Blood. 2007;109(8):3489–3495. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
