

Long-term quality of life in critically ill patients with acute kidney injury treated with renal replacement therapy: a matched cohort study
- PMID: 26250830
- PMCID: PMC4527359
- DOI: 10.1186/s13054-015-1004-8
Long-term quality of life in critically ill patients with acute kidney injury treated with renal replacement therapy: a matched cohort study
Abstract
Introduction: Acute kidney injury (AKI) is a common complication in intensive care unit (ICU) patients and is associated with increased morbidity and mortality. We compared long-term outcome and quality of life (QOL) in ICU patients with AKI treated with renal replacement therapy (RRT) with matched non-AKI-RRT patients.
Methods: Over 1 year, consecutive adult ICU patients were included in a prospective cohort study. AKI-RRT patients alive at 1 year and 4 years were matched with non-AKI-RRT survivors from the same cohort in a 1:2 (1 year) and 1:1 (4 years) ratio based on gender, age, Acute Physiology and Chronic Health Evaluation II score, and admission category. QOL was assessed by the EuroQoL-5D and the Short Form-36 survey before ICU admission and at 3 months, 1 and 4 years after ICU discharge.
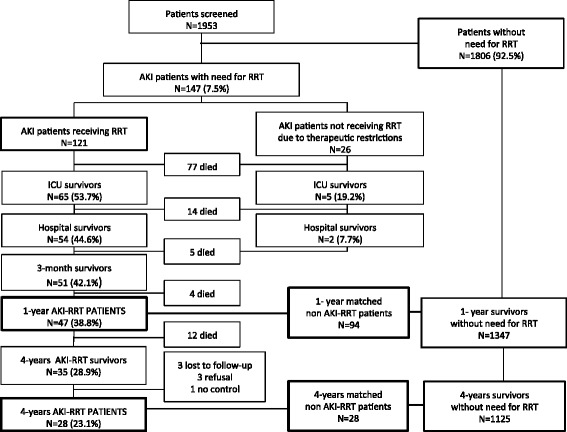
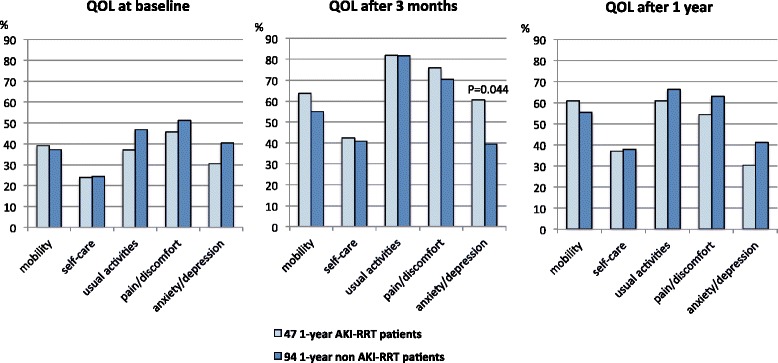
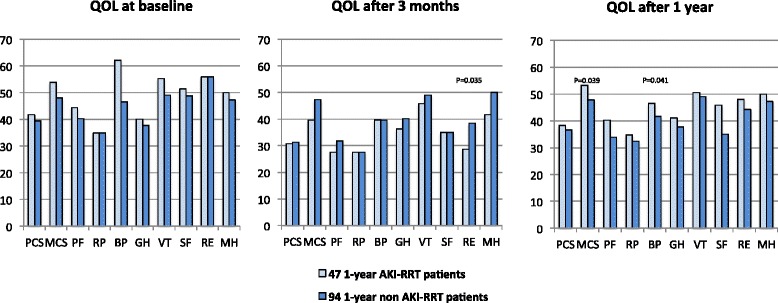
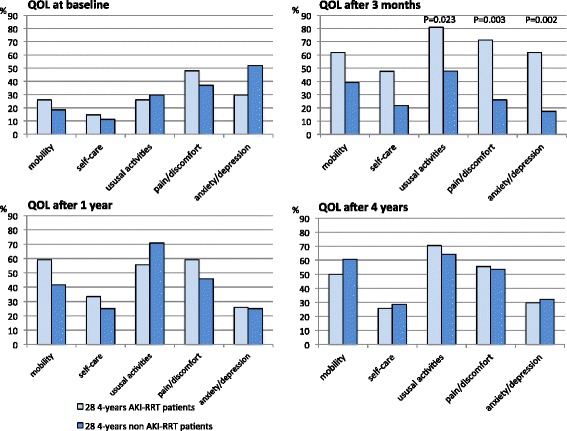
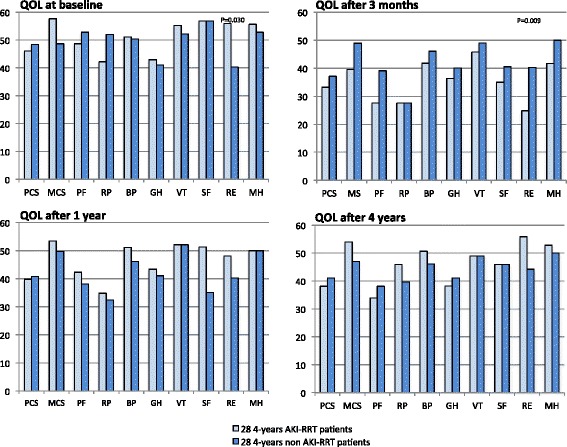
Results: Of 1953 patients, 121 (6.2%) had AKI-RRT. AKI-RRT hospital survivors (44.6%; N = 54) had a 1-year and 4-year survival rate of 87.0% (N = 47) and 64.8% (N = 35), respectively. Forty-seven 1-year AKI-RRT patients were matched with 94 1-year non-AKI-RRT patients. Of 35 4-year survivors, three refused further cooperation, three were lost to follow-up, and one had no control. Finally, 28 4-year AKI-RRT patients were matched with 28 non-AKI-RRT patients. During ICU stay, 1-year and 4-year AKI-RRT patients had more organ dysfunction compared to their respective matches (Sequential Organ Failure Assessment scores 7 versus 5, P < 0.001, and 7 versus 4, P < 0.001). Long-term QOL was, however, comparable between both groups but lower than in the general population. QOL decreased at 3 months, improved after 1 and 4 years but remained under baseline level. One and 4 years after ICU discharge, 19.1% and 28.6% of AKI-RRT survivors remained RRT-dependent, respectively, and 81.8% and 71% of them were willing to undergo ICU admission again if needed.
Conclusion: In long-term critically ill AKI-RRT survivors, QOL was comparable to matched long-term critically ill non-AKI-RRT survivors, but lower than in the general population. The majority of AKI-RRT patients wanted to be readmitted to the ICU when needed, despite a higher severity of illness compared to matched non-AKI-RRT patients, and despite the fact that one quarter had persistent dialysis dependency.
Figures
Similar articles
-
RIFLE-based data collection/management system applied to a prospective cohort multicenter Italian study on the epidemiology of acute kidney injury in the intensive care unit.Blood Purif. 2011;31(1-3):159-71. doi: 10.1159/000322161. Epub 2011 Jan 10. Blood Purif. 2011. PMID: 21228585
-
Long-term outcome in ICU patients with acute kidney injury treated with renal replacement therapy: a prospective cohort study.Crit Care. 2016 Aug 12;20(1):256. doi: 10.1186/s13054-016-1409-z. Crit Care. 2016. PMID: 27520553 Free PMC article.
-
Prospective multicenter study on epidemiology of acute kidney injury in the ICU: a critical care nephrology Italian collaborative effort (NEFROINT).Minerva Anestesiol. 2011 Nov;77(11):1072-83. Epub 2011 May 11. Minerva Anestesiol. 2011. PMID: 21597441
-
Long-term outcome after acute kidney injury in critically-ill patients.Acta Clin Belg. 2007;62 Suppl 2:337-40. doi: 10.1179/acb.2007.076. Acta Clin Belg. 2007. PMID: 18283995 Review.
-
Effects of renal replacement therapy on renal recovery after acute kidney injury.Nephron Clin Pract. 2014;127(1-4):35-41. doi: 10.1159/000363671. Epub 2014 Sep 24. Nephron Clin Pract. 2014. PMID: 25343818 Review.
Cited by
-
Health-related quality-of-life among survivors of acute kidney injury in the intensive care unit: a systematic review.Intensive Care Med. 2016 Feb;42(2):137-46. doi: 10.1007/s00134-015-4151-0. Epub 2015 Dec 1. Intensive Care Med. 2016. PMID: 26626062
-
Economic Analysis of Renal Replacement Therapy Modality in Acute Kidney Injury Patients With Fluid Overload.Crit Care Explor. 2023 Jun 5;5(6):e0921. doi: 10.1097/CCE.0000000000000921. eCollection 2023 Jun. Crit Care Explor. 2023. PMID: 37637357 Free PMC article.
-
Issues of Acute Kidney Injury Staging and Management in Sepsis and Critical Illness: A Narrative Review.Int J Mol Sci. 2017 Jun 28;18(7):1387. doi: 10.3390/ijms18071387. Int J Mol Sci. 2017. PMID: 28657585 Free PMC article. Review.
-
Quality of life following hospitalization-associated acute kidney injury in children.J Nephrol. 2018 Apr;31(2):249-256. doi: 10.1007/s40620-017-0450-6. Epub 2017 Nov 18. J Nephrol. 2018. PMID: 29151251 Free PMC article.
-
Survive or thrive after ICU: what's the score?Ann Intensive Care. 2023 May 19;13(1):43. doi: 10.1186/s13613-023-01140-x. Ann Intensive Care. 2023. PMID: 37202549 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
