

Cost-Utility Analysis of Mechanical Thrombectomy Using Stent Retrievers in Acute Ischemic Stroke
- PMID: 26251241
- PMCID: PMC4542565
- DOI: 10.1161/STROKEAHA.115.009396
Cost-Utility Analysis of Mechanical Thrombectomy Using Stent Retrievers in Acute Ischemic Stroke
Abstract
Background and purpose: Recently, 5 randomized controlled trials demonstrated the benefit of endovascular therapy compared with intravenous tissue-type plasminogen activator in acute stroke. Economic evidence evaluating stent retrievers is limited. We compared the cost-effectiveness of intravenous tissue-type plasminogen activator alone versus mechanical thrombectomy and intravenous tissue-type plasminogen activator as a bridging therapy in eligible patients in the UK National Health Service.
Methods: A model-based cost-utility analysis was performed using a lifetime horizon. A Markov model was constructed and populated with probabilities, outcomes, and cost data from published sources, including 1-way and probabilistic sensitivity analysis.
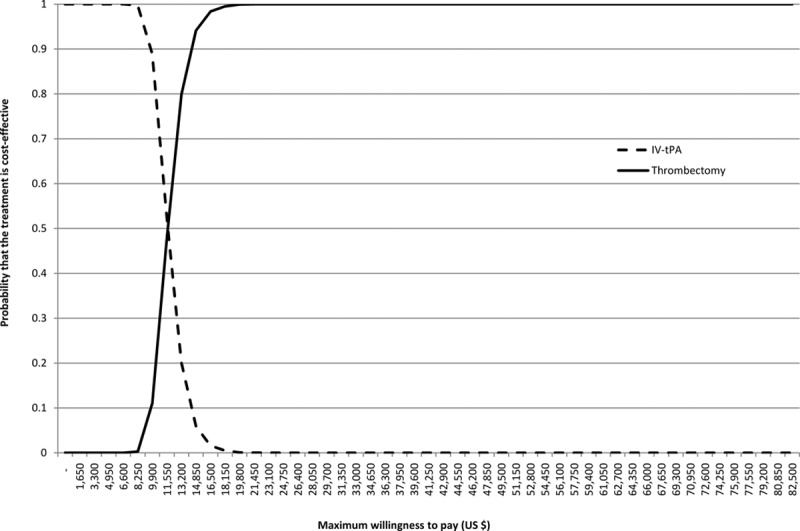
Results: Mechanical thrombectomy was more expensive than intravenous tissue-type plasminogen activator, but it improved quality-adjusted life expectancy. The incremental cost per (quality-adjusted life year) gained of mechanical thrombectomy over a 20 year period was $11 651 (£7061). The probabilistic sensitivity analysis demonstrated that thrombectomy had a 100% probability of being cost-effective at the minimum willingness to pay for a quality-adjusted life year commonly used in United Kingdom.
Conclusions: Although the upfront costs of thrombectomy are high, the potential quality-adjusted life year gains mean this intervention is cost-effective. This is an important factor for consideration in deciding whether to commission this intervention.
Keywords: cost-effectiveness; stents; stroke; thrombectomy; tissue-type plasminogen activator.
© 2015 The Authors.
Figures


References
-
- Adamson J, Beswick A, Ebrahim S. Is stroke the most common cause of disability? J Stroke Cerebrovasc Dis. 2004;13:171–177. doi: 10.1016/j.jstrokecerebrovasdis.2004.06.003. - PubMed
-
- Truelsen T, Piechowski-Jóźwiak B, Bonita R, Mathers C, Bogousslavsky J, Boysen G. Stroke incidence and prevalence in Europe: a review of available data. Eur J Neurol. 2006;13:581–598. doi: 10.1111/j.1468-1331.2006.01138.x. - PubMed
-
- Saka O, McGuire A, Wolfe C. Cost of stroke in the United Kingdom. Age Ageing. 2009;38:27–32. doi: 10.1093/ageing/afn281. - PubMed
-
- Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Blaha MJ, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics–2014 update: a report from the American Heart Association. Circulation. 2014;129:e28–e292. doi: 10.1161/01.cir.0000441139.02102.80. - PMC - PubMed
-
- Hacke W, Kaste M, Bluhmki E, Brozman M, Dávalos A, Guidetti D, et al. ECASS Investigators. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008;359:1317–1329. doi: 10.1056/NEJMoa0804656. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
