

Differentiation between Cystic Pituitary Adenomas and Rathke Cleft Cysts: A Diagnostic Model Using MRI
- PMID: 26251436
- PMCID: PMC7965051
- DOI: 10.3174/ajnr.A4387
Differentiation between Cystic Pituitary Adenomas and Rathke Cleft Cysts: A Diagnostic Model Using MRI
Abstract
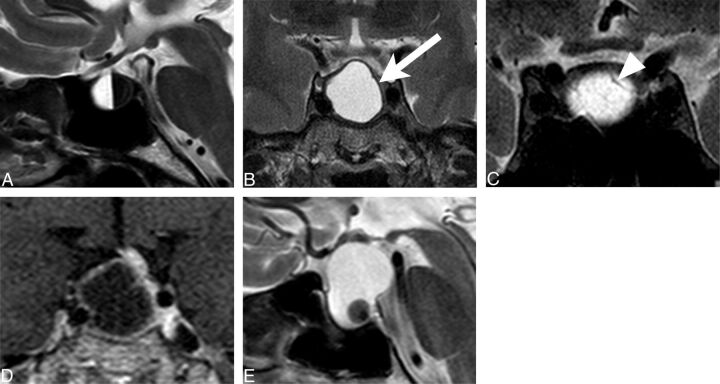
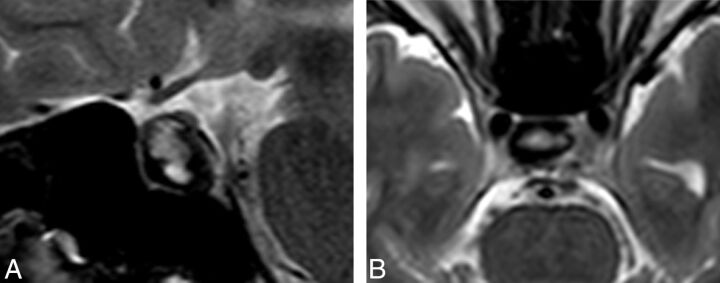
Background and purpose: Cystic pituitary adenomas may mimic Rathke cleft cysts when there is no solid enhancing component found on MR imaging, and preoperative differentiation may enable a more appropriate selection of treatment strategies. We investigated the diagnostic potential of MR imaging features to differentiate cystic pituitary adenomas from Rathke cleft cysts and to develop a diagnostic model.
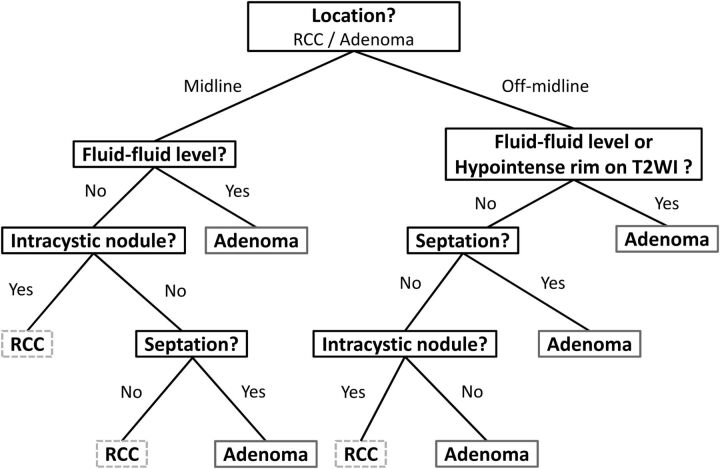
Materials and methods: This retrospective study included 54 patients with a cystic pituitary adenoma (40 women; mean age, 37.7 years) and 28 with a Rathke cleft cyst (18 women; mean age, 31.5 years) who underwent MR imaging followed by surgery. The following imaging features were assessed: the presence or absence of a fluid-fluid level, a hypointense rim on T2-weighted images, septation, an off-midline location, the presence or absence of an intracystic nodule, size change, and signal change. On the basis of the results of logistic regression analysis, a diagnostic tree model was developed to differentiate between cystic pituitary adenomas and Rathke cleft cysts. External validation was performed for an additional 16 patients with a cystic pituitary adenoma and 8 patients with a Rathke cleft cyst.
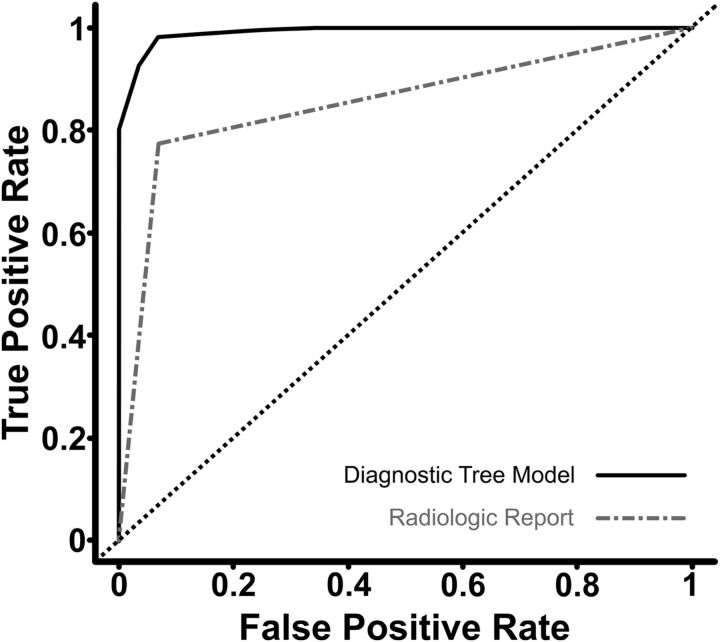
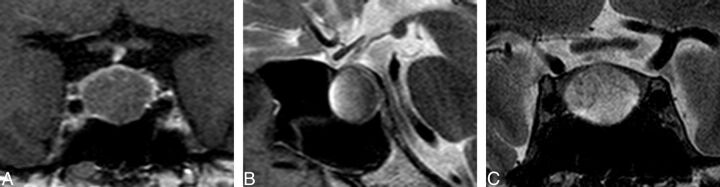
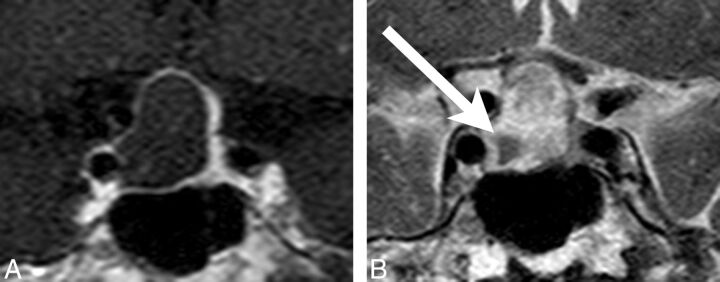
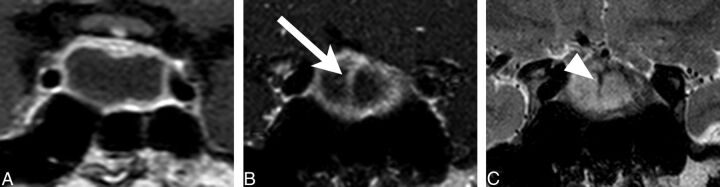
Results: The presence of a fluid-fluid level, a hypointense rim on T2-weighted images, septation, and an off-midline location were more common with pituitary adenomas, whereas the presence of an intracystic nodule was more common with Rathke cleft cysts. Multiple logistic regression analysis showed that cystic pituitary adenomas and Rathke cleft cysts can be distinguished on the basis of the presence of a fluid-fluid level, septation, an off-midline location, and the presence of an intracystic nodule (P = .006, .032, .001, and .023, respectively). Among 24 patients in the external validation population, 22 were classified correctly on the basis of the diagnostic tree model used in this study.
Conclusions: A systematic approach using this diagnostic tree model can be helpful in distinguishing cystic pituitary adenomas from Rathke cleft cysts.
© 2015 by American Journal of Neuroradiology.
Figures
Comment in
-
Hemorrhagic Pituitary Adenoma versus Rathke Cleft Cyst: A Frequent Dilemma.AJNR Am J Neuroradiol. 2016 Mar;37(3):E27-8. doi: 10.3174/ajnr.A4653. Epub 2015 Dec 17. AJNR Am J Neuroradiol. 2016. PMID: 26680456 Free PMC article. No abstract available.
-
Reply.AJNR Am J Neuroradiol. 2016 Mar;37(3):E29. doi: 10.3174/ajnr.A4668. Epub 2015 Dec 17. AJNR Am J Neuroradiol. 2016. PMID: 26680458 Free PMC article. No abstract available.
References
-
- Semple PL, Webb MK, de Villiers JC, et al. . Pituitary apoplexy. Neurosurgery 2005;56:65–72; discussion 72–73 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical