

Usefulness and feasibility of measuring ionized calcium in haemodialysis patients
- PMID: 26251703
- PMCID: PMC4515894
- DOI: 10.1093/ckj/sfv039
Usefulness and feasibility of measuring ionized calcium in haemodialysis patients
Abstract
Background: Measuring blood calcium level is recommended in haemodialysis (HD) patients. The Kidney Disease Improving Global Outcomes position states that the measurement of ionized calcium (ICa) level is preferred, but in the clinical setting, due to technical difficulties, total calcium (tCa) level is preferred to ICa.
Aim: The aim of this study was to test the possibility of delayed ICa analysis using frozen serum, and so to identify the factors associated with predialysis ICa level and compare the ability of tCa and Alb-Ca to predict ICa level and finally to compare the survival rate according to the three calcium measurements.
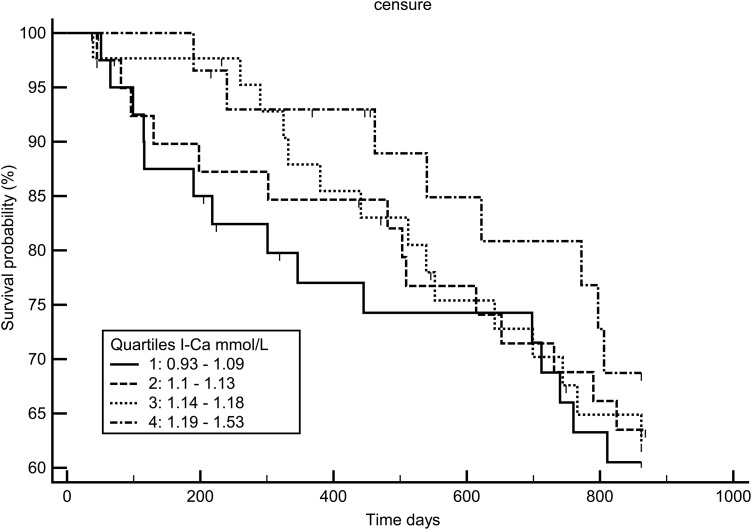
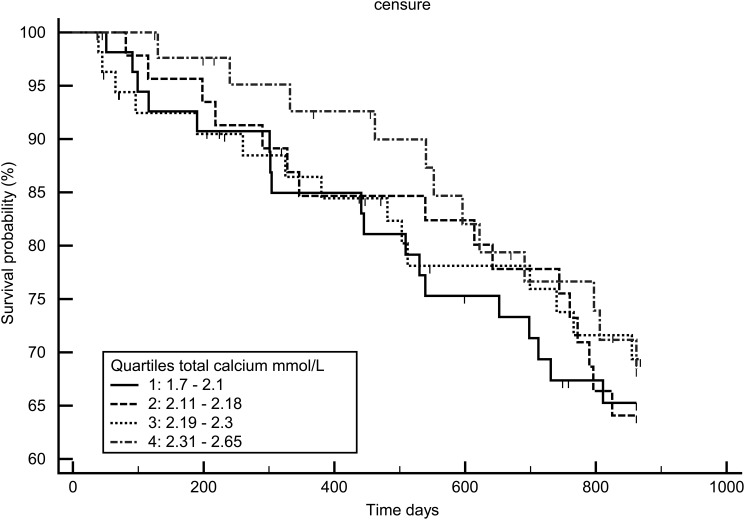
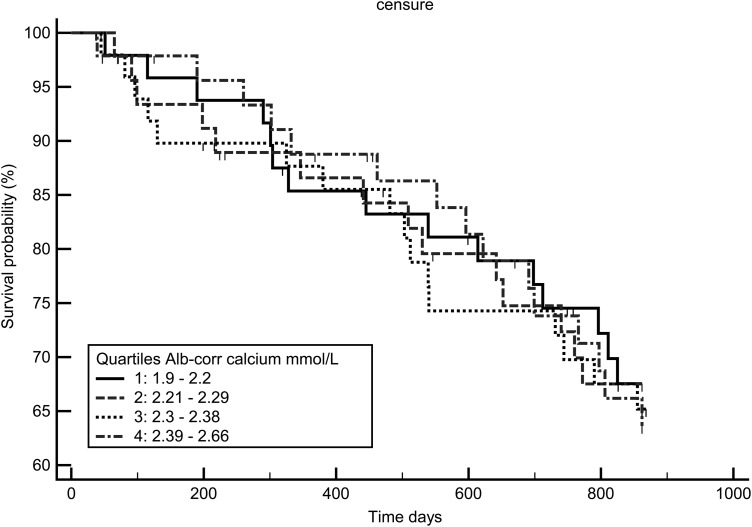
Methods: All prevalent HD patients, dialysed by a native AV fistula in a 3 × 4 to 3 × 8 h schedule, had their predialysis ICa, tCa and Alb-Ca levels and usual mid-week biology recorded. Intergroup comparisons between ICa quartile were performed. Bland-Altman plots and linear regression were used to assess the differences between 30 fresh and frozen samples. Survival analyses were performed using ICa and tCa levels.
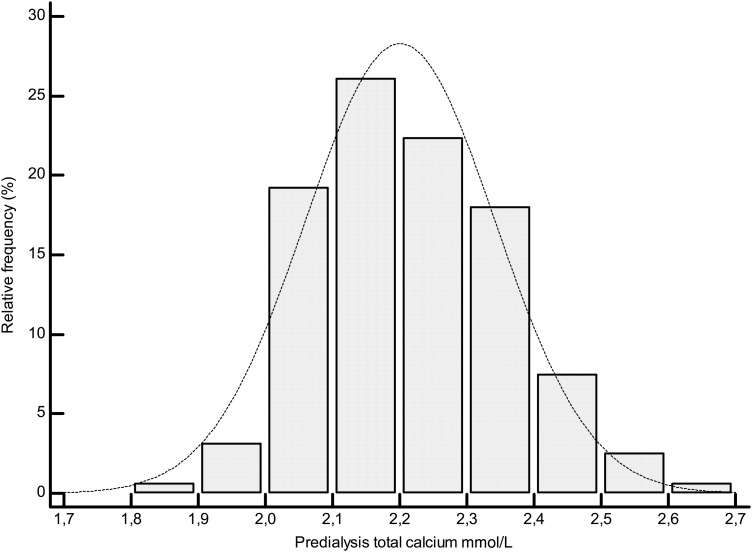
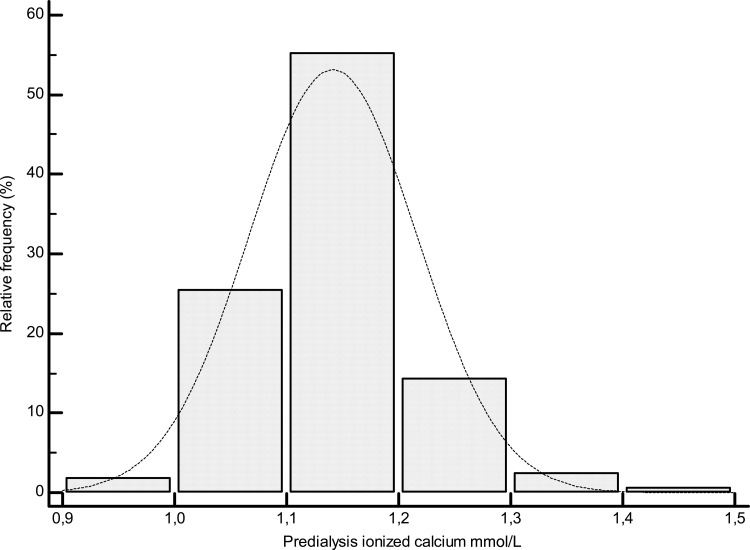
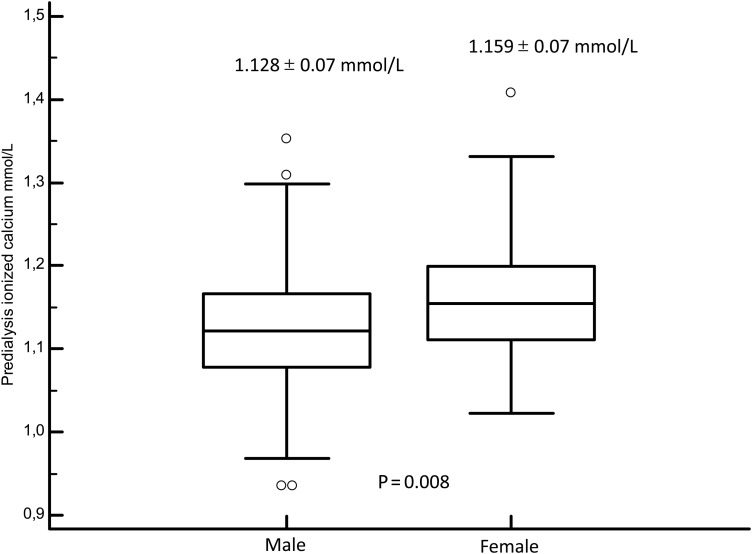
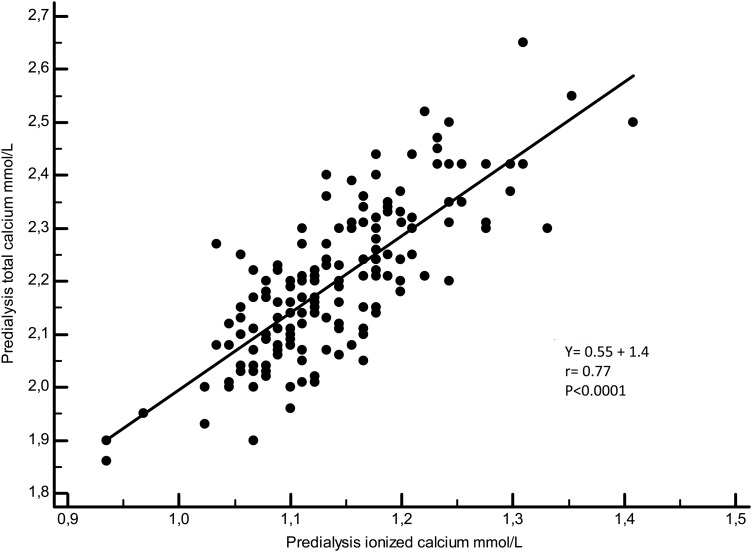
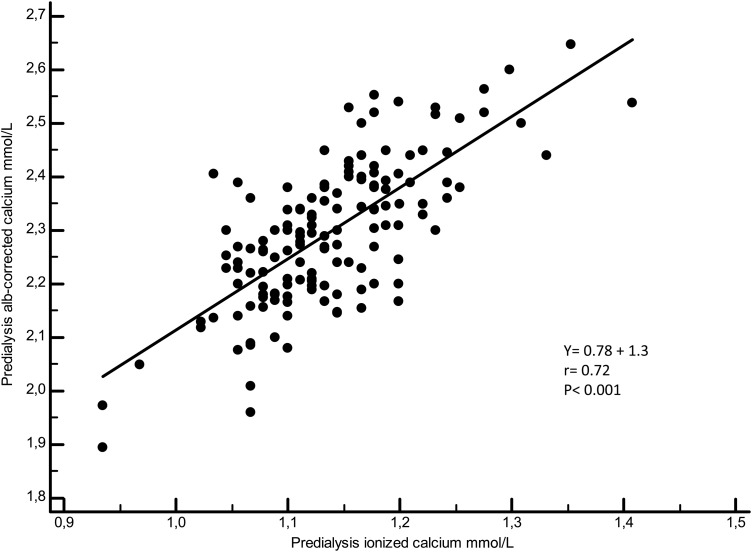
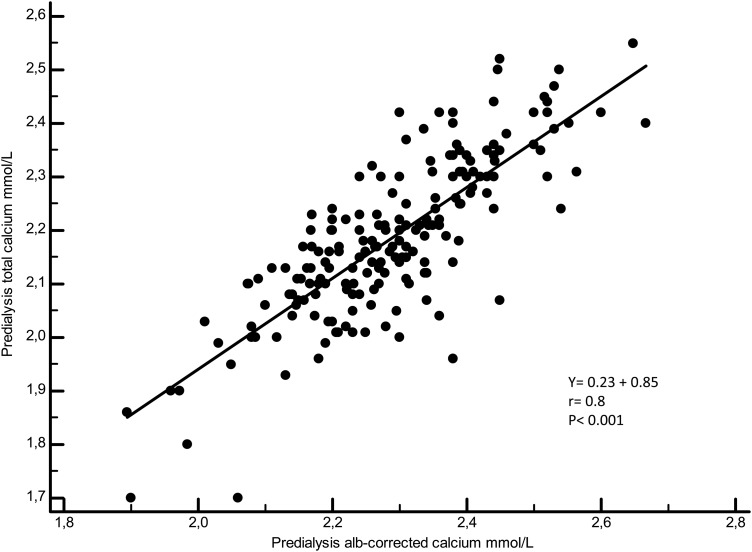
Results: Comparing fresh blood and frozen serum samples, linear regression (y = 0.98 + 0.02, r = 0.961) showed that the two methods were quite identical with the same mean ICa value (1.1 ± 0.1 mmol/L, P = 0.45). A total of 160 HD patients were included in the study. Hypocalcaemia, using ICa values, was highly prevalent in our population (40%) whereas hypercalcaemia was observed only in three cases (1.8%). In predicting ICa hypocalcaemia (<1.12 mmol/L, n = 64), the use of tCa was accurate in 48.4% of patients, and the use of Alb-Ca was accurate in only 17.2% of patients; tCa was not a predictive factor for hypercalcaemia (ICa > 1.32 mmol/L, n = 3); Alb-Ca value predicted hypercalcaemia in 2/3 of the patients. In predicting normocalcaemia, the use of tCa values was correct in 92.4% of patients and the use of Alb-Ca values in 88.1% of patients; only younger age (P = 0.03) and female sex (P = 0.01) were associated with higher ICa quartile. None of the three calcium measures was significantly associated with survival rate using log-rank and Cox models adjusted for age, dialysis vintage, diabetes and sex.
Conclusion: In the present study, we report that (1) delayed ICa measure is feasible in dialysis patients using a freezing technique, (2) hypocalcaemia is highly prevalent in HD patients and poorly predicted by Alb-Ca level, (3) the main factor associated with ICa level is sex of the individual and (4) calcaemia is not associated with survival rate using any of the three methods.
Keywords: frozen sample; haemodialysis; ionized calcium; survival analysis.
Figures
References
-
- Akerstrom G, Hellman P, Hessman O, et al. Parathyroid glands in calcium regulation and human disease. Ann N Y Acad Sci 2005; 1040: 53–58 - PubMed
-
- Clase CM, Norman GL, Beecroft ML, et al. Albumin-corrected calcium and ionized calcium in stable haemodialysis patients. Nephrol Dial Transplant 2000; 15: 1841–1846 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
