

Malignant Transformation of Grade II Ependymoma in a 2-Year-Old Child: Case Report
- PMID: 26251794
- PMCID: PMC4520988
- DOI: 10.1055/s-0035-1549311
Malignant Transformation of Grade II Ependymoma in a 2-Year-Old Child: Case Report
Abstract
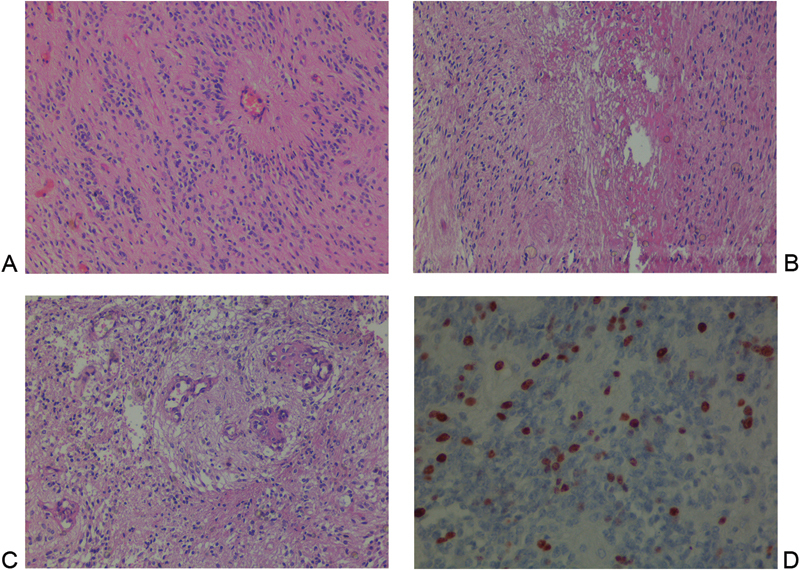
Ependymomas are central nervous system neoplasms that account for a third of all posterior fossa tumors in children. The most common location for infratentorial ependymoma is within the fourth ventricle. We present a case report of malignant transformation of an infratentorial grade II ependymoma in a 2-year-old child who presented with vomiting and visual disturbance. An infratentorial brain tumor in the left cerebellar area was totally removed, and the initial pathologic diagnosis was grade II ependymoma. The tumor recurred aggressively 1 year later; subtotal removal and adjuvant chemotherapy were performed. After a second operation, a histopathologic study was performed. The second specimen was defined as a grade III anaplastic ependymoma. Transformation to grade III anaplastic ependymoma is possible for a grade II ependymoma but very rare. The diagnosis of the anaplastic variant of intracranial ependymomas is difficult. Surgical treatment remains the mainstay of the treatment for all cases. Ependymomas in young infants have a worse prognosis than older children, so we need individual clinical evaluation and close follow-up of such cases. This article highlights the requirement of a close follow-up for grade II ependymomas for anaplastic transformation.
Keywords: brain; central nervous system; ependymoma; malignant transformation; neoplasm.
Figures


References
-
- McLaughlin M P, Marcus R B Jr, Buatti J M. et al.Ependymoma: results, prognostic factors and treatment recommendations. Int J Radiat Oncol Biol Phys. 1998;40(4):845–850. - PubMed
-
- Schiffer D, Giordana M T. Prognosis of ependymoma. Childs Nerv Syst. 1998;14(8):357–361. - PubMed
-
- Applegate G L, Marymont M H. Intracranial ependymomas: a review. Cancer Invest. 1998;16(8):588–593. - PubMed
-
- Lefton D R, Pinto R S, Martin S W. MRI features of intracranial and spinal ependymomas. Pediatr Neurosurg. 1998;28(2):97–105. - PubMed
-
- Gerszten P C, Pollack I F, Martínez A J, Lo K H, Janosky J, Albright A L. Intracranial ependymomas of childhood. Lack of correlation of histopathology and clinical outcome. Pathol Res Pract. 1996;192(6):515–522. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources