

Glioblastoma Multiforme in a Patient with Isolated Hemimegalencephaly
- PMID: 26251796
- PMCID: PMC4520982
- DOI: 10.1055/s-0035-1554929
Glioblastoma Multiforme in a Patient with Isolated Hemimegalencephaly
Abstract
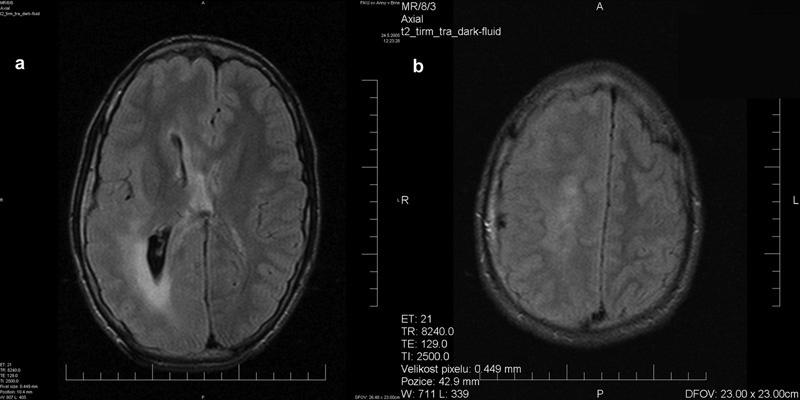
We present an exceptional case of a patient with hemimegalencephaly and secondary intractable epilepsy treated with vagus nerve stimulation (VNS) and subsequent glioblastoma development in the hemimegalencephalic hemisphere 6 years after surgery. VNS (at age 18 years) led to a 60% reduction of intractable seizures. However, symptoms of intracranial hypertension suddenly occurred 6 years after surgery. A computed tomography scan revealed a brain tumor in the hemimegalencephalic hemisphere. Pathologic examination confirmed glioblastoma multiforme. The genetic background of hemimegalencephaly is discussed here, with attention paid to the available data about the malignant transformation of malformations of cortical development (MCDs). The case points to the need for adequate clinical and radiologic follow-up care for patients with MCDs including hemimegalencephaly.
Keywords: epilepsy; glioblastoma multiforme; hemimegalencephaly; malformations of cortical development.
Figures


Similar articles
-
Malformations of cortical development (MCDs) and epilepsy: experience from a tertiary care center in south India.Seizure. 2010 Apr;19(3):147-52. doi: 10.1016/j.seizure.2010.01.005. Epub 2010 Feb 9. Seizure. 2010. PMID: 20144553
-
Hemimegalencephaly with intractable epilepsy: A case report.J Pak Med Assoc. 2017 Sep;67(9):1444-1446. J Pak Med Assoc. 2017. PMID: 28924292
-
Hemimegalencephaly in an adult with normal intellectual function and mild epilepsy.Dev Med Child Neurol. 2012 Mar;54(3):284-6. doi: 10.1111/j.1469-8749.2011.04136.x. Epub 2011 Dec 21. Dev Med Child Neurol. 2012. PMID: 22188130
-
Vagus nerve stimulation for seizures.Arch Med Res. 2000 May-Jun;31(3):300-3. doi: 10.1016/s0188-4409(00)00060-6. Arch Med Res. 2000. PMID: 11036181 Review.
-
Hemimegalencephaly without epilepsy: case report.Childs Nerv Syst. 2014 Sep;30(9):1617-9. doi: 10.1007/s00381-014-2392-9. Epub 2014 Mar 4. Childs Nerv Syst. 2014. PMID: 24589886 Review.
Cited by
-
Vagus nerve stimulation: Novel concept for the treatment of glioblastoma and solid cancers by cytokine (interleukin-6) reduction, attenuating the SASP, enhancing tumor immunity.Brain Behav Immun Health. 2024 Sep 17;42:100859. doi: 10.1016/j.bbih.2024.100859. eCollection 2024 Dec. Brain Behav Immun Health. 2024. PMID: 39512605 Free PMC article. Review.
-
miR-181a-5p inhibits the proliferation and invasion of drug-resistant glioblastoma cells by targeting F-box protein 11 expression.Oncol Lett. 2020 Nov;20(5):235. doi: 10.3892/ol.2020.12098. Epub 2020 Sep 14. Oncol Lett. 2020. PMID: 32968457 Free PMC article.
-
Ultracentrifugation versus kit exosome isolation: nanoLC-MS and other tools reveal similar performance biomarkers, but also contaminations.Future Sci OA. 2018 Nov 9;5(1):FSO359. doi: 10.4155/fsoa-2018-0088. eCollection 2019 Jan. Future Sci OA. 2018. PMID: 30652024 Free PMC article.
-
Evolution of epilepsy in hemimegalencephaly from infancy to adulthood: Case report and review of the literature.Epilepsy Behav Case Rep. 2017 Mar 1;7:45-48. doi: 10.1016/j.ebcr.2017.02.002. eCollection 2017. Epilepsy Behav Case Rep. 2017. PMID: 28377884 Free PMC article.
References
-
- Kuzniecky R J, Jackson G D. New York, NY: Raven Press; 1995. Magnetic Resonance in Epilepsy.
-
- Di Rocco C, Battaglia D, Pietrini D, Piastra M, Massimi L. Hemimegalencephaly: clinical implications and surgical treatment. Childs Nerv Syst. 2006;22(08):852–866. - PubMed
-
- Manoranjan B, Provias J P. Hemimegalencephaly: a fetal case with neuropathological confirmation and review of the literature. Acta Neuropathol. 2010;120(01):117–130. - PubMed
-
- Perry M S, Duchowny M. Cambridge, UK: Cambridge University Press; 2011. Hemimegalencephaly; pp. 289–292.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases