

Real-time prediction of inpatient length of stay for discharge prioritization
- PMID: 26253131
- PMCID: PMC4954620
- DOI: 10.1093/jamia/ocv106
Real-time prediction of inpatient length of stay for discharge prioritization
Abstract
Objective: Hospitals are challenged to provide timely patient care while maintaining high resource utilization. This has prompted hospital initiatives to increase patient flow and minimize nonvalue added care time. Real-time demand capacity management (RTDC) is one such initiative whereby clinicians convene each morning to predict patients able to leave the same day and prioritize their remaining tasks for early discharge. Our objective is to automate and improve these discharge predictions by applying supervised machine learning methods to readily available health information.
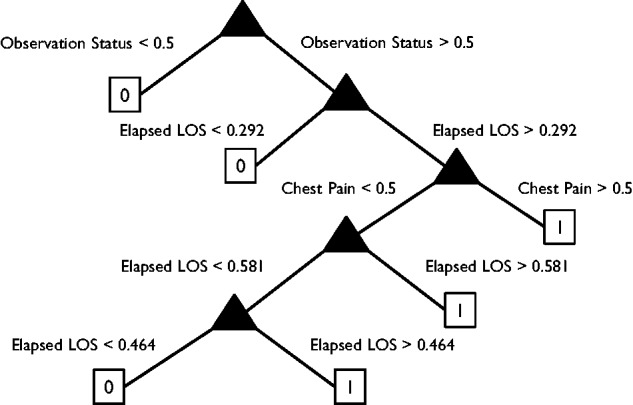
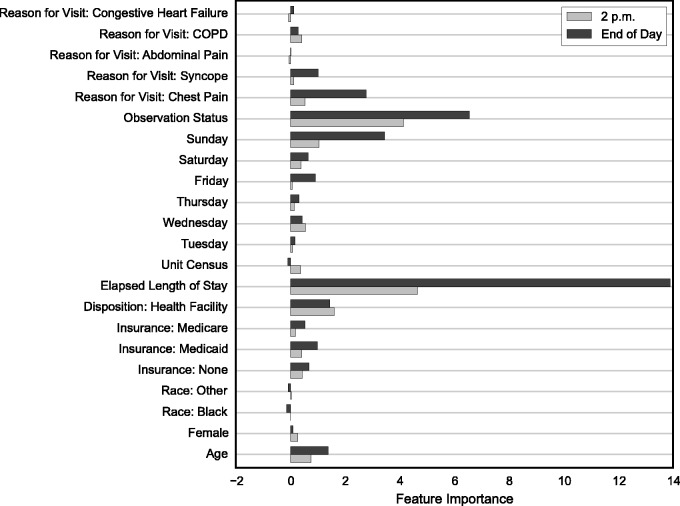
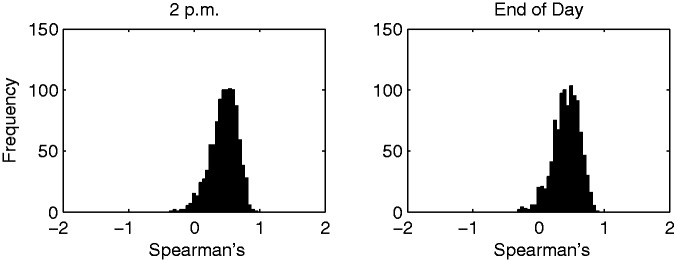
Materials and methods: The authors use supervised machine learning methods to predict patients' likelihood of discharge by 2 p.m. and by midnight each day for an inpatient medical unit. Using data collected over 8000 patient stays and 20 000 patient days, the predictive performance of the model is compared to clinicians using sensitivity, specificity, Youden's Index (i.e., sensitivity + specificity - 1), and aggregate accuracy measures.
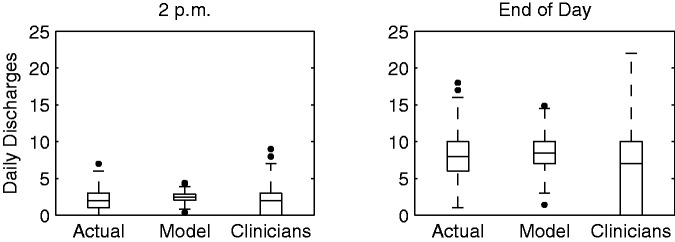
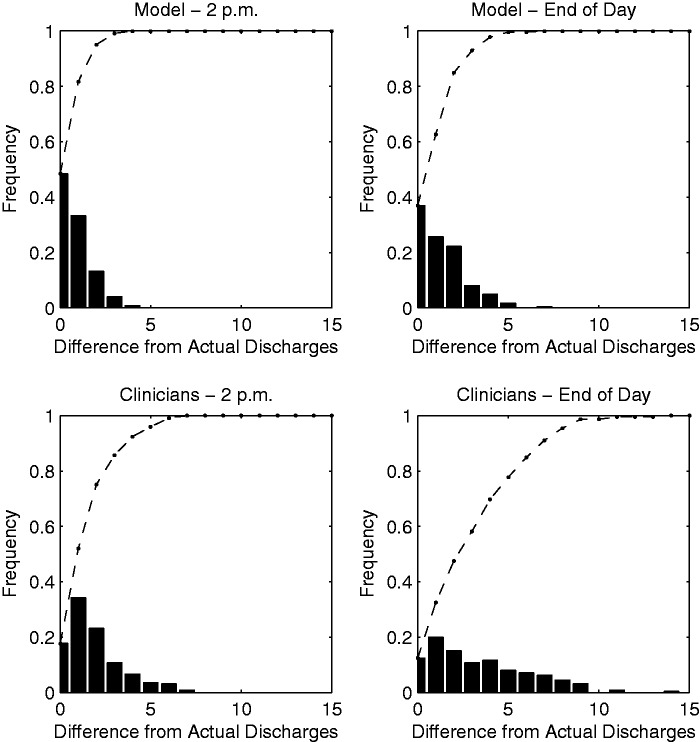
Results: The model compared to clinician predictions demonstrated significantly higher sensitivity (P < .01), lower specificity (P < .01), and a comparable Youden Index (P > .10). Early discharges were less predictable than midnight discharges. The model was more accurate than clinicians in predicting the total number of daily discharges and capable of ranking patients closest to future discharge.
Conclusions: There is potential to use readily available health information to predict daily patient discharges with accuracies comparable to clinician predictions. This approach may be used to automate and support daily RTDC predictions aimed at improving patient flow.
Keywords: length of stay; machine learning; operational forecasting; patient flow.
© The Author 2015. Published by Oxford University Press on behalf of the American Medical Informatics Association. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academies Press; 2001. - PubMed
-
- Bernstein SL, Aronsky D, Duseja R, et al. The effect of emergency department crowding on clinically oriented outcomes. Acad Emerg Med. 2000;16(1):1–10. - PubMed
-
- Levin S, Dittus R, Aronsky D, et al. Evaluating the effects of increasing surgical volume on emergency department patient access. BMJ Qual Saf. 2011;20:146–152. - PubMed
-
- Ryckman FC, Yelton PA, Anneken AM, et al. Redesigning intensive care unit flow using variability management to improve access and safety. Jt Comm J Qual Patient Safety. 2009;35:535–543. - PubMed
-
- Compton DW, Ganjiang G, Reid PP, et al. Building a Better Delivery System: A New Engineering/Health Care Partnership. Washington, DC: National Academies Press; 2005. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
