

Personalizing colonoscopy screening for elderly individuals based on screening history, cancer risk, and comorbidity status could increase cost effectiveness
- PMID: 26253304
- PMCID: PMC4631390
- DOI: 10.1053/j.gastro.2015.07.042
Personalizing colonoscopy screening for elderly individuals based on screening history, cancer risk, and comorbidity status could increase cost effectiveness
Abstract
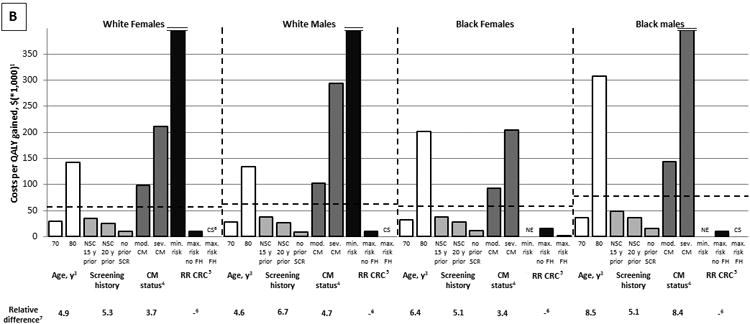
Background & aims: Colorectal cancer (CRC) screening decisions for elderly individuals are often made primarily on the basis of age, whereas other factors that influence the effectiveness and cost effectiveness of screening are often not considered. We investigated the relative importance of factors that could be used to identify elderly individuals most likely to benefit from CRC screening and determined the maximum ages at which screening remains cost effective based on these factors.
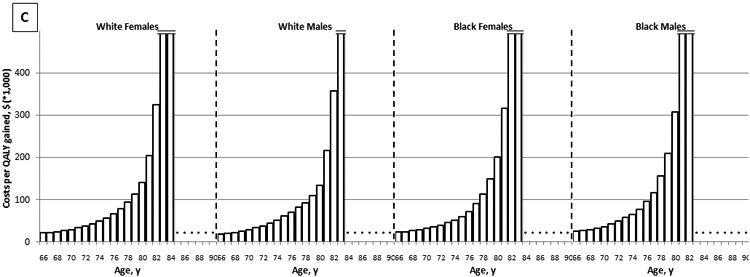
Methods: We used a microsimulation model (Microsimulation Screening Analysis-Colon) calibrated to the incidence of CRC in the United States and the prevalence of adenomas reported in autopsy studies to determine the appropriate age at which to stop colonoscopy screening in 19,200 cohorts (of 10 million individuals), defined by sex, race, screening history, background risk for CRC, and comorbidity status. We applied a willingness-to-pay threshold of $100,000 per quality-adjusted life-year (QALY) gained.
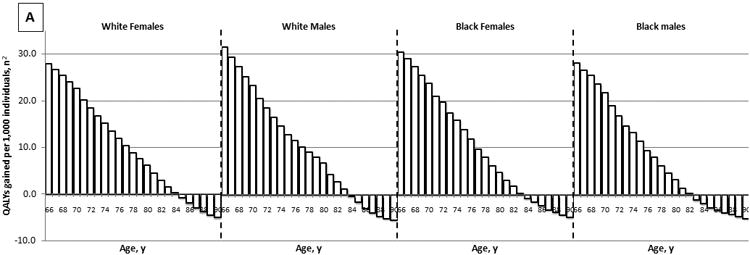
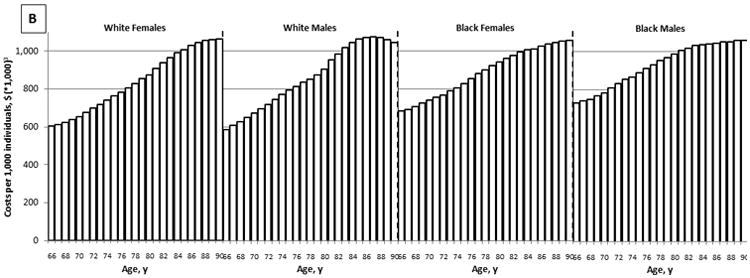
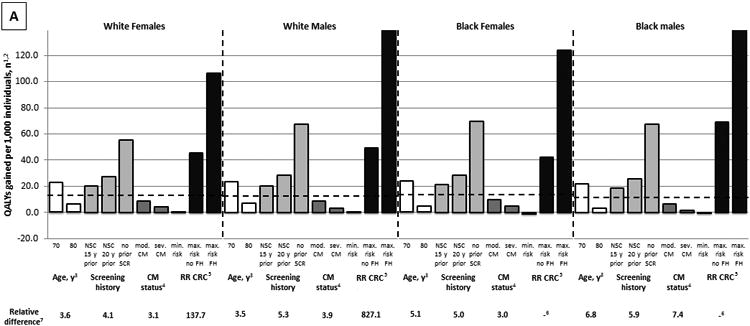
Results: Less intensive screening history, higher background risk for CRC, and fewer comorbidities were associated with cost-effective screening at older ages. Sex and race had only a small effect on the appropriate age to stop screening. For some individuals likely to be screened in current practice (for example, 74-year-old white women with moderate comorbidities, half the average background risk for CRC, and negative findings from a screening colonoscopy 10 years previously), screening resulted in a loss of QALYs, rather than a gain. For some individuals unlikely to be screened in current practice (for example, 81-year-old black men with no comorbidities, an average background risk for CRC, and no previous screening), screening was highly cost effective. Although screening some previously screened, low-risk individuals was not cost effective even when they were 66 years old, screening some healthy, high-risk individuals remained cost effective until they reached the age of 88 years old.
Conclusions: The current approach to CRC screening in elderly individuals, in which decisions are often based primarily on age, is inefficient, resulting in underuse of screening for some and overuse of screening for others. CRC screening could be more effective and cost effective if individual factors for each patient are considered.
Keywords: Colon Cancer Screening; Individualized Care; MISCAN; Tumor.
Copyright © 2015 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Colorectal cancer screening is cost-effective in the elderly who have had less intense prior screening, high baseline risk of colorectal cancer and less comorbidities.Evid Based Med. 2016 Oct;21(5):182. doi: 10.1136/ebmed-2015-110359. Epub 2016 Aug 23. Evid Based Med. 2016. PMID: 27555637 No abstract available.
References
-
- Screening for colorectal cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2008;149:627–37. - PubMed
-
- Levin B, Lieberman DA, McFarland B, et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. Gastroenterology. 2008;134:1570–95. - PubMed
-
- Qaseem A, Denberg TD, Hopkins RH, Jr, et al. Screening for colorectal cancer: a guidance statement from the American College of Physicians. Ann Intern Med. 2012;156:378–86. - PubMed
-
- Rex DK, Johnson DA, Anderson JC, et al. American College of Gastroenterology guidelines for colorectal cancer screening 2009 [corrected] Am J Gastroenterol. 2009;104:739–50. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
