

Clinical and Angiographic Predictors of Microvascular Dysfunction in ST-Segment Elevation Myocardial Infarction
- PMID: 26256965
- PMCID: PMC4541652
- DOI: 10.3349/ymj.2015.56.5.1235
Clinical and Angiographic Predictors of Microvascular Dysfunction in ST-Segment Elevation Myocardial Infarction
Abstract
Purpose: We aimed to discover clinical and angiographic predictors of microvascular dysfunction using the index of microcirculatory resistance (IMR) in patients with ST-segment elevation myocardial infarction (STEMI).
Materials and methods: We enrolled 113 patients with STEMI (age, 56±11 years; 95 men) who underwent primary percutaneous coronary intervention (PCI). The IMR was measured with a pressure sensor/thermistor-tipped guidewire after primary PCI. The patients were divided into three groups based on IMR values: Low IMR [<18 U (12.9±2.6 U), n=38], Mid IMR [18-31 U (23.9±4.0 U), n=38], and High IMR [>31 U (48.1±17.1 U), n=37].
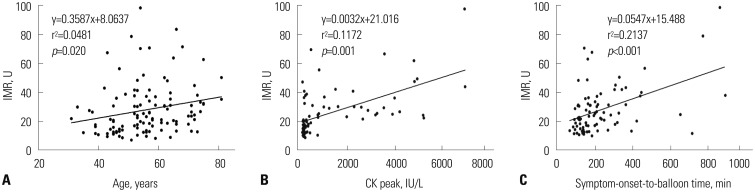
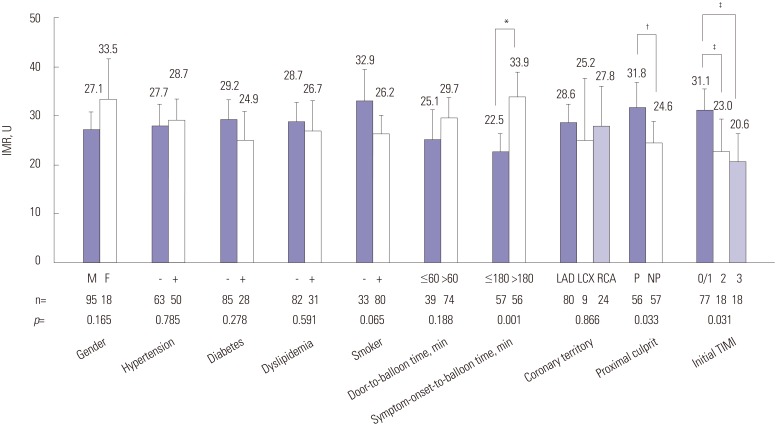
Results: The age of the Low IMR group was significantly lower than that of the Mid and High IMR groups. The door-to-balloon time was <90 minutes in all patients, and it was not significantly different between groups. Meanwhile, the symptom-onset-to-balloon time was significantly longer in the High IMR group, compared to the Mid and Low IMR groups (p<0.001). In the high IMR group, the culprit lesion was found in a proximal location significantly more often than in a non-proximal location (p=0.008). In multivariate regression analysis, age and symptom-onset-to-balloon time were independent determinants of a high IMR (p=0.013 and p=0.003, respectively).
Conclusion: Our data suggest that age and symptom-onset-to-balloon time might be the major predictors of microvascular dysfunction in STEMI patients with a door-to-balloon time of <90 minutes.
Keywords: Microvascular dysfunction; ST-segment elevation myocardial infarction; doorto-balloon time; index of microcirculatory resistance; symptom-onset-to-balloon time.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- Fearon WF, Balsam LB, Farouque HM, Caffarelli AD, Robbins RC, Fitzgerald PJ, et al. Novel index for invasively assessing the coronary microcirculation. Circulation. 2003;107:3129–3132. - PubMed
-
- Leung DY, Leung M. Non-invasive/invasive imaging: significance and assessment of coronary microvascular dysfunction. Heart. 2011;97:587–595. - PubMed
-
- Niccoli G, Burzotta F, Galiuto L, Crea F. Myocardial no-reflow in humans. J Am Coll Cardiol. 2009;54:281–292. - PubMed
-
- Gibson CM, Cannon CP, Murphy SA, Ryan KA, Mesley R, Marble SJ, et al. Relationship of TIMI myocardial perfusion grade to mortality after administration of thrombolytic drugs. Circulation. 2000;101:125–130. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
