

Telepsychiatrists' Medication Treatment Strategies in the Children's Attention-Deficit/Hyperactivity Disorder Telemental Health Treatment Study
- PMID: 26258927
- PMCID: PMC5069727
- DOI: 10.1089/cap.2015.0017
Telepsychiatrists' Medication Treatment Strategies in the Children's Attention-Deficit/Hyperactivity Disorder Telemental Health Treatment Study
Abstract
Objective: The purpose of this study was to examine the prescribing strategies that telepsychiatrists used to provide pharmacologic treatment in the Children's Attention-Deficit/Hyperactivity Disorder (ADHD) Telemental Health Treatment Study (CATTS).
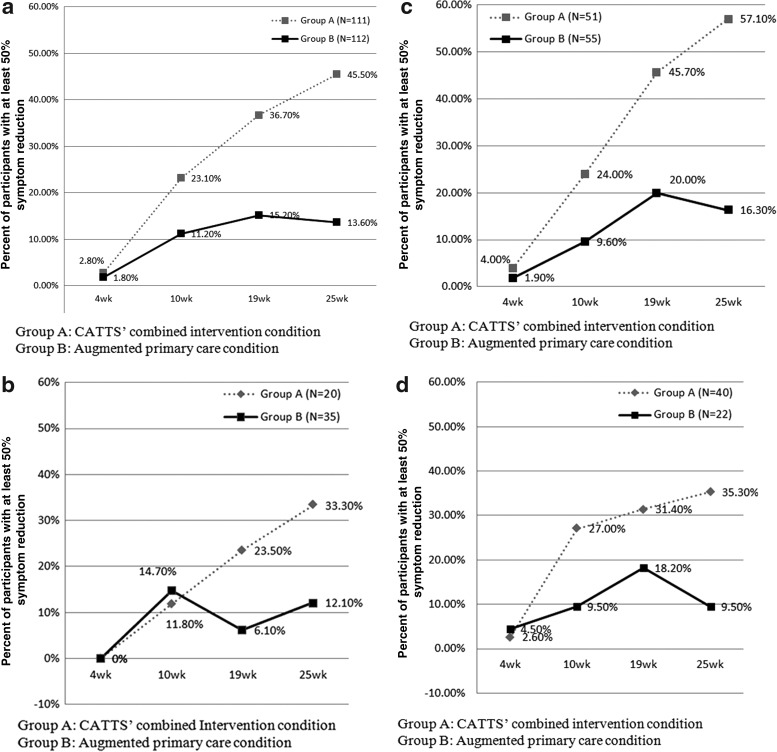
Methods: CATTS was a randomized controlled trial that demonstrated the superiority of a telehealth service delivery model for the treatment of ADHD with combined pharmacotherapy and behavior training (n=111), compared with management in primary care augmented with a telepsychiatry consultation (n=112). A diagnosis of ADHD was established with the Computerized Diagnostic Interview Schedule for Children (CDISC), and comorbidity for oppositional defiant disorder (ODD) and anxiety disorders (AD) was established using the CDISC and the Child Behavior Checklist. Telepsychiatrists used the Texas Children's Medication Algorithm Project (TCMAP) for ADHD to guide pharmacotherapy and the treat-to-target model to encourage their assertive medication management to a predetermined goal of 50% reduction in ADHD-related symptoms. We assessed whether telepsychiatrists' decision making about making medication changes was associated with baseline ADHD symptom severity, comorbidity, and attainment of the treat-to-target goal.
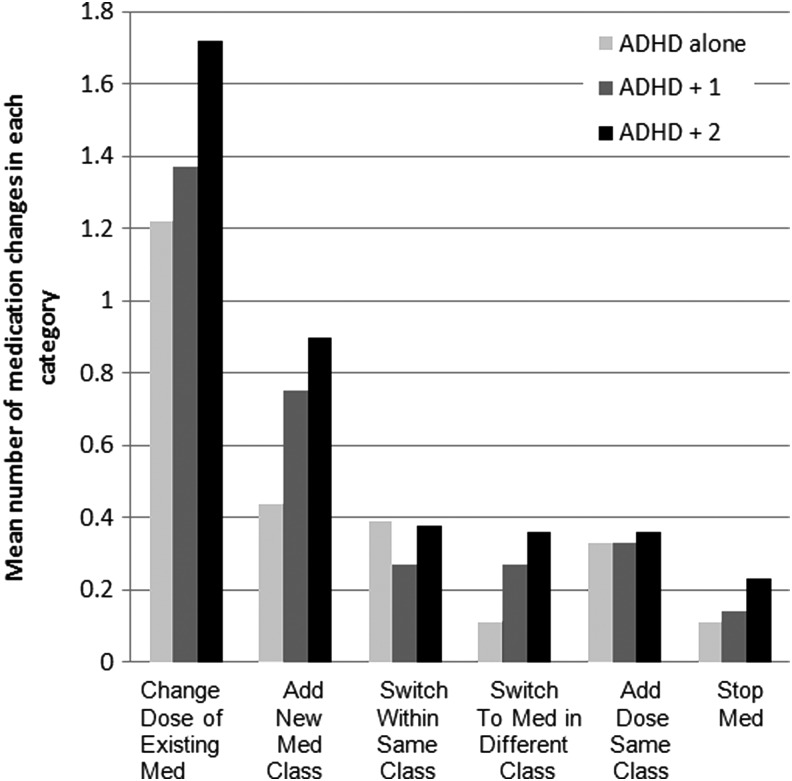
Results: Telepsychiatrists showed high fidelity (91%) to their chosen algorithms in medication management. At the end of the trial, the CATTS intervention showed 46.0% attainment of the treat-to-target goal compared with 13.6% for the augmented primary care condition, and significantly greater attainment of the goal by comorbidity status for the ADHD with one and ADHD with two comorbidities groups. Telepsychiatrists' were more likely to decide to make medication adjustments for youth with higher baseline ADHD severity and the presence of disorders comorbid with ADHD. Multiple mixed methods regression analyses controlling for baseline ADHD severity and comorbidity status indicated that the telepsychiatrists also based their decision making session to session on attainment of the treat-to-target goal.
Conclusions: Telepsychiatry is an effective service delivery model for providing pharmacotherapy for ADHD, and the CATTS telepsychiatrists showed high fidelity to evidence-based protocols.
Trial registration: ClinicalTrials.gov NCT00830700.
Keywords: evidence-based telepsychiatry; telemental health; telepsychiatrists’ adherence; telepsychiatry; telepsychiatry for ADHD; telepsychiatry outcomes.
Figures
References
-
- Achenbach TM, Rescorla LA: Manual for the ASEBA School-Age Forms & Profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, & Families; 2001
-
- American Academy of Child and Adolescent Psychiatry: Practice parameter for the assessment and treatment of children and adolescents with attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry 46:894–921, 2007 - PubMed
-
- American Academy of Pediatrics, Subcommittee on Attention-Deficit/Hyperactivity Disorder and Steering Committee on Quality Improvement and Management: ADHD: Clinical practice guideline for diagnosis, evaluation, and treatment of attention-deficit/hyperactivity disorder in children and adolescents. Pediatrics 128:1007–1022, 2011 - PMC - PubMed
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.: Washington, DC: American Psychiatric Association; 1994
-
- Buitelaar JK, Montgomery SA, van Zwieten–Boot BJ: Attention deficit hyperactivity disorder: Guidelines for investigating efficacy of pharmacological intervention. Eur Neuropsychopharmacol 13:297–304, 2003 - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
