

Bioelectrical impedance vector analysis in critically ill patients: a prospective, clinician-blinded investigation
- PMID: 26260579
- PMCID: PMC4531396
- DOI: 10.1186/s13054-015-1009-3
Bioelectrical impedance vector analysis in critically ill patients: a prospective, clinician-blinded investigation
Abstract
Introduction: Assessment of fluid status in critically ill patients is challenging. We aimed to assess the feasibility and validity of bioelectrical impedance vector analysis (BIVA) as a measure of hydration in critically ill patients.
Methods: We performed twice-daily BIVA measurements and fluid balance calculations and recorded physiological variables in mechanically ventilated patients within 24 h of intensive care unit (ICU) admission for up to 5 days. Treating clinicians were blinded to BIVA results.
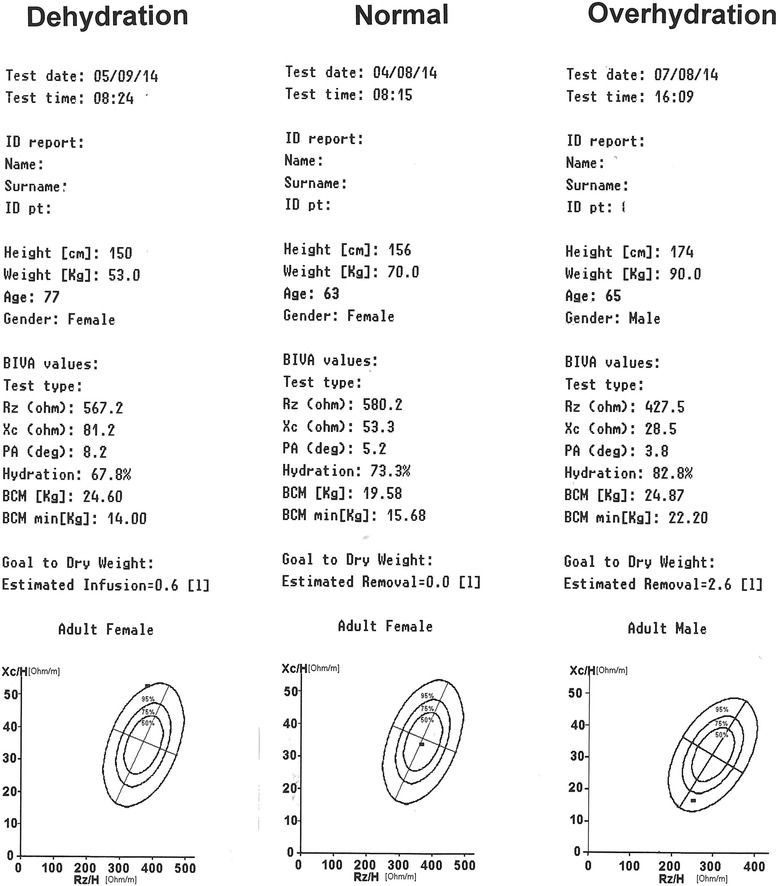
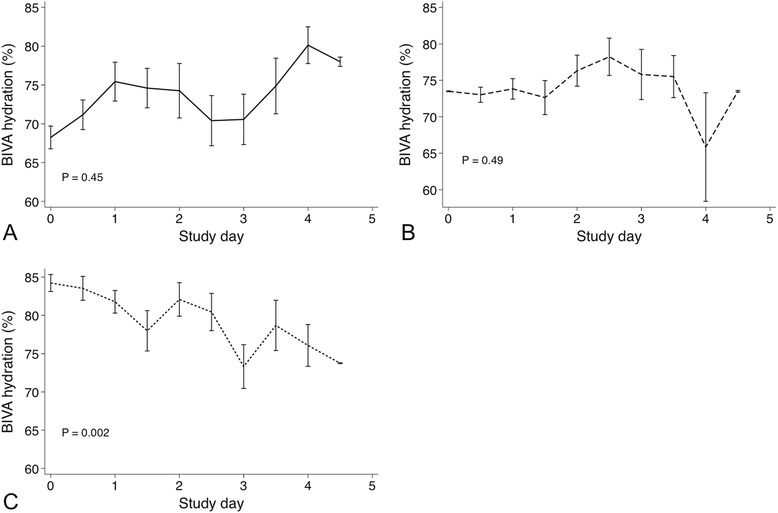
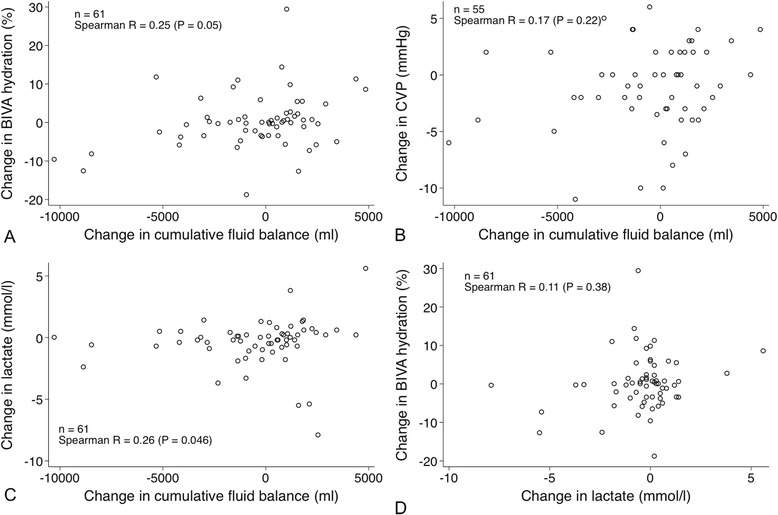
Results: We performed 344 BIVA measurements in 61 patients. According to BIVA, 14 patients (23%) were dehydrated, 22 (36%) were normally hydrated and 25 (41%) were overhydrated upon ICU admission. Patients with normal BIVA hydration were less sick, had fewer comorbidities and had less deranged physiology than patients found to be dehydrated or overhydrated with BIVA. Cumulative fluid balance increased in patients found to be dehydrated with BIVA by a mean of 3.4±2.2 L, whereas in patients found to be overhydrated with BIVA, it decreased by a mean of 4.5±6.9 L. In patients found to be normally hydrated with BIVA, fluid balance remained unchanged. BIVA-defined hydration increased with 1 L (median change 1.5%, P =0.09) or 2 L (median change 0.7%, P =0.09) of calculated fluid gains. BIVA-defined hydration decreased (median change -0.8%, P =0.02) with a negative cumulative fluid balance of >2 L. BIVA-defined hydration between first and last measurement correlated with the corresponding change in fluid balance (ρ =0.25, P =0.05).
Conclusions: BIVA is feasible in critically ill patients. Its validity is supported by the observed characteristics of patients with different degrees of BIVA hydration upon admission and by different fluid management of such patients by blinded clinicians. The sensitivity of repeated BIVA hydration measurements to detect fluid accumulation or fluid balance changes <2 L was low, however. These contradictory findings provide the rational basis for studies of BIVA-assisted fluid management in ICU patients.
Figures


Comment in
-
Bioelectrical impedance vector analysis in the critically ill: cool tool or just another 'toy'?Crit Care. 2015 Nov 11;19:387. doi: 10.1186/s13054-015-1110-7. Crit Care. 2015. PMID: 26556282 Free PMC article.
References
-
- Kumar A, Anel R, Bunnell E, Habet K, Zanotti S, Marshall S, et al. Pulmonary artery occlusion pressure and central venous pressure fail to predict ventricular filling volume, cardiac performance, or the response to volume infusion in normal subjects. Crit Care Med. 2004;32:691–9. doi: 10.1097/01.CCM.0000114996.68110.C9. - DOI - PubMed
-
- Perren A, Markmann M, Merlani G, Marone C, Merlani P. Fluid balance in critically ill patients: should we really rely on it? Minerva Anesthesiol. 2011;77:802–11. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
