

Atrophy patterns in early clinical stages across distinct phenotypes of Alzheimer's disease
- PMID: 26260856
- PMCID: PMC4692964
- DOI: 10.1002/hbm.22927
Atrophy patterns in early clinical stages across distinct phenotypes of Alzheimer's disease
Abstract
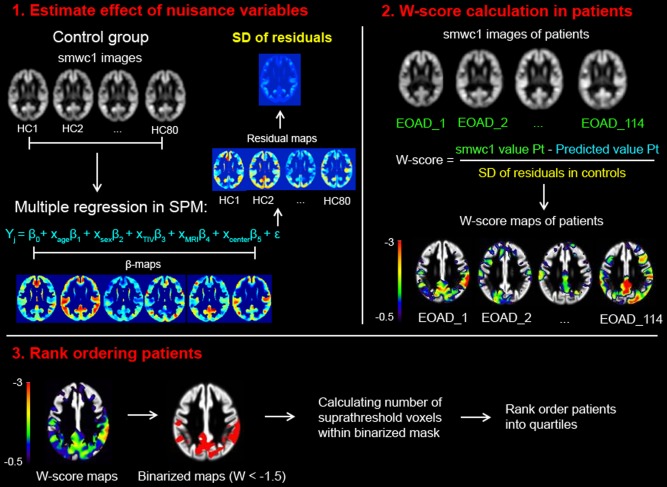
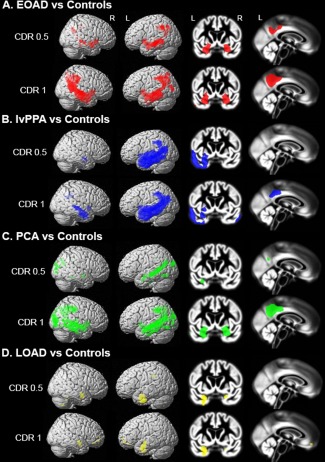
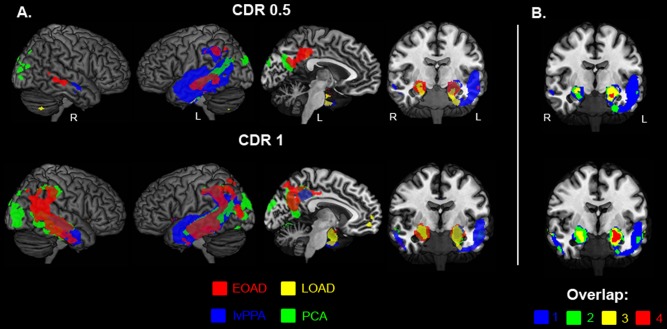
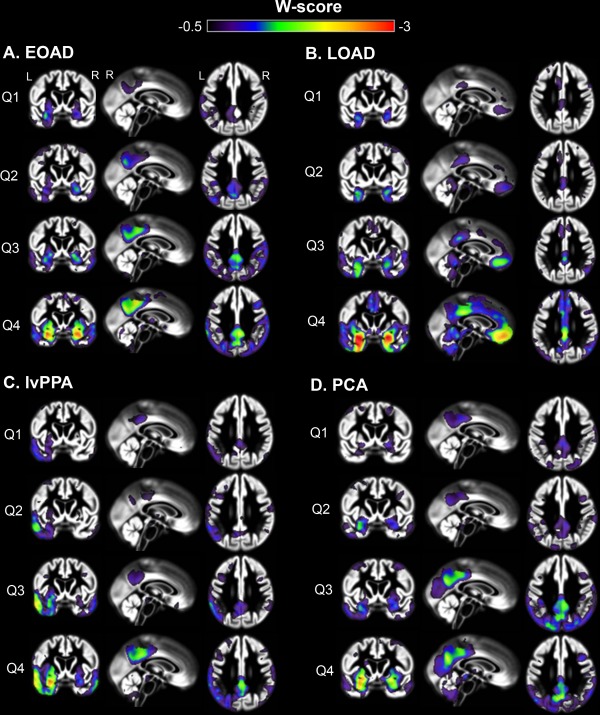
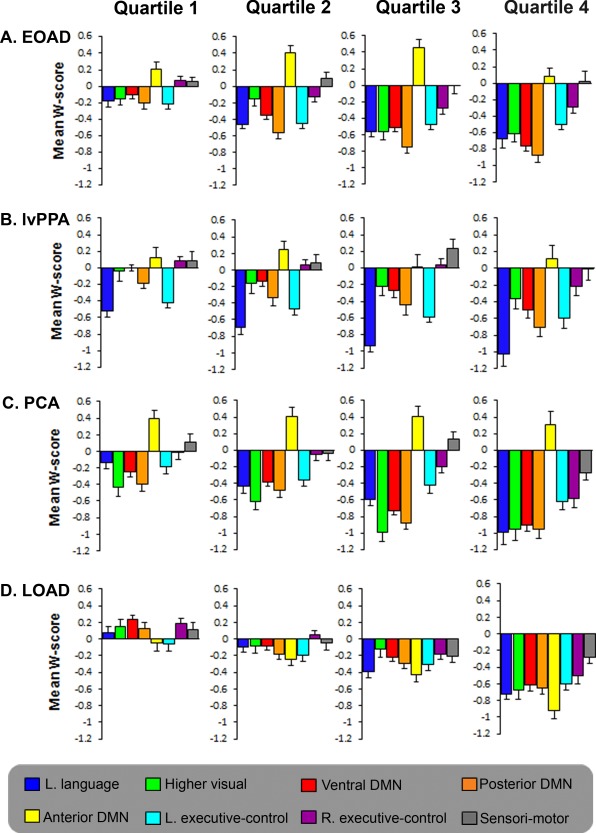
Alzheimer's disease (AD) can present with distinct clinical variants. Identifying the earliest neurodegenerative changes associated with each variant has implications for early diagnosis, and for understanding the mechanisms that underlie regional vulnerability and disease progression in AD. We performed voxel-based morphometry to detect atrophy patterns in early clinical stages of four AD phenotypes: Posterior cortical atrophy (PCA, "visual variant," n=93), logopenic variant primary progressive aphasia (lvPPA, "language variant," n=74), and memory-predominant AD categorized as early age-of-onset (EOAD, <65 years, n=114) and late age-of-onset (LOAD, >65 years, n=114). Patients with each syndrome were stratified based on: (1) degree of functional impairment, as measured by the clinical dementia rating (CDR) scale, and (2) overall extent of brain atrophy, as measured by a neuroimaging approach that sums the number of brain voxels showing significantly lower gray matter volume than cognitively normal controls (n=80). Even at the earliest clinical stage (CDR=0.5 or bottom quartile of overall atrophy), patients with each syndrome showed both common and variant-specific atrophy. Common atrophy across variants was found in temporoparietal regions that comprise the posterior default mode network (DMN). Early syndrome-specific atrophy mirrored functional brain networks underlying functions that are uniquely affected in each variant: Language network in lvPPA, posterior cingulate cortex-hippocampal circuit in amnestic EOAD and LOAD, and visual networks in PCA. At more advanced stages, atrophy patterns largely converged across AD variants. These findings support a model in which neurodegeneration selectively targets both the DMN and syndrome-specific vulnerable networks at the earliest clinical stages of AD.
Keywords: Alzheimer's disease; atrophy; default mode network; early-onset dementia; language; logopenic variant primary progressive aphasia; magnetic resonance imaging (MRI); memory; posterior cortical atrophy; vision; voxel-based morphometry.
© 2015 Wiley Periodicals, Inc.
Figures
References
-
- Albert MS, DeKosky ST, Dickson D, Dubois B, Feldman HH, Fox NC, Gamst A, Holtzman DM, Jagust WJ, Petersen RC, Snyder PJ, Carrillo MC, Thies B, Phelps CH (2011): The diagnosis of mild cognitive impairment due to Alzheimer's disease: recommendations from the National Institute on Aging‐Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement 7:270–279. - PMC - PubMed
-
- Alladi S, Xuereb J, Bak T, Nestor P, Knibb J, Patterson K, Hodges JR (2007): Focal cortical presentations of Alzheimer's disease. Brain 130:2636–2645. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
