

Solid Predominant Histologic Subtype in Resected Stage I Lung Adenocarcinoma Is an Independent Predictor of Early, Extrathoracic, Multisite Recurrence and of Poor Postrecurrence Survival
- PMID: 26261257
- PMCID: PMC4554749
- DOI: 10.1200/JCO.2015.60.9818
Solid Predominant Histologic Subtype in Resected Stage I Lung Adenocarcinoma Is an Independent Predictor of Early, Extrathoracic, Multisite Recurrence and of Poor Postrecurrence Survival
Abstract
Purpose: To examine the significance of the proposed International Association for the Study of Lung Cancer, American Thoracic Society, and European Respiratory Society (IASLC/ATS/ERS) histologic subtypes of lung adenocarcinoma for patterns of recurrence and, among patients who recur following resection of stage I lung adenocarcinoma, for postrecurrence survival (PRS).
Patients and methods: We reviewed patients with stage I lung adenocarcinoma who had undergone complete surgical resection from 1999 to 2009 (N = 1,120). Tumors were subtyped by using the IASLC/ATS/ERS classification. The effects of the dominant subtype on recurrence and, among patients who recurred, on PRS were investigated.
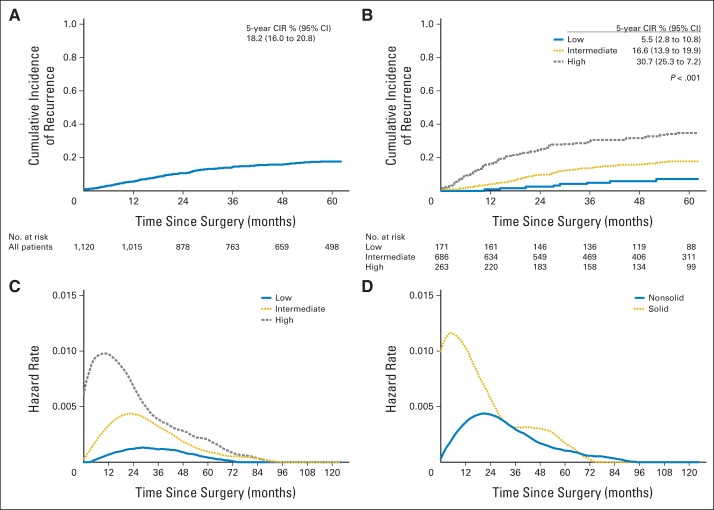
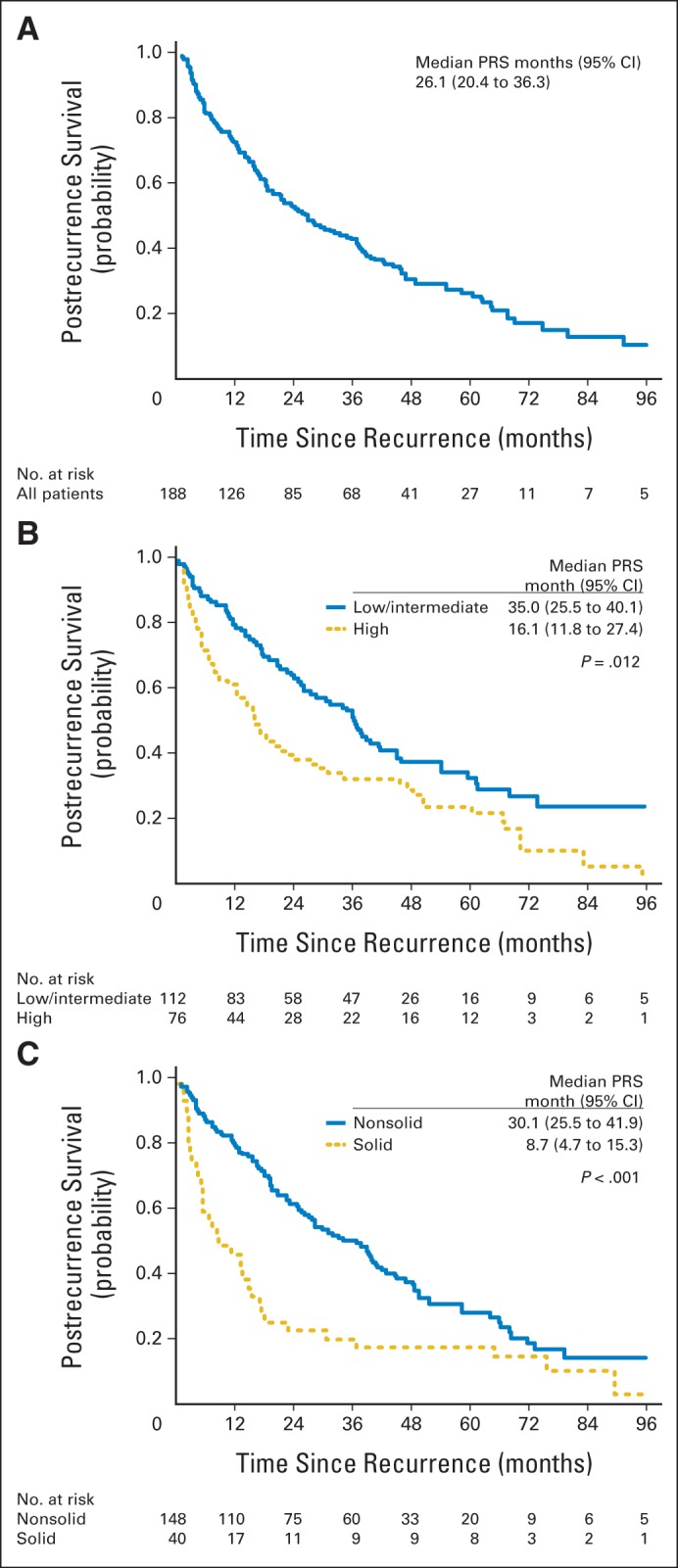
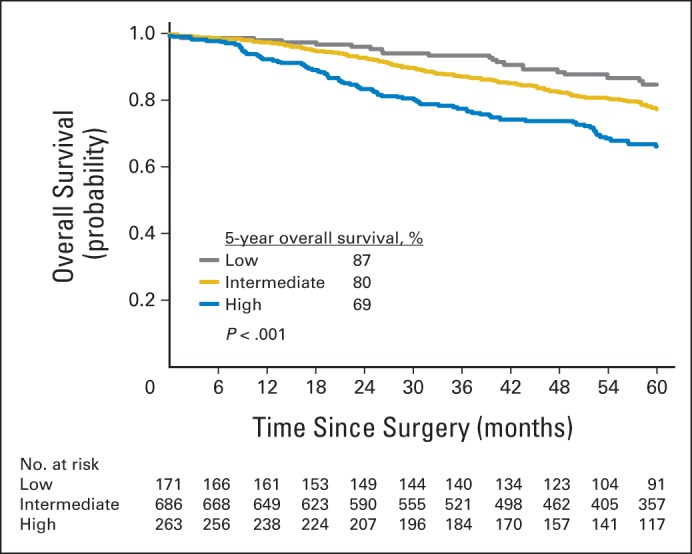
Results: Of 1,120 patients identified, 188 had recurrent disease, 103 of whom died as a result of lung cancer. Among patients who recurred, 2-year PRS was 45%, and median PRS was 26.1 months. Compared with patients with nonsolid tumors, patients with solid predominant tumors had earlier (P = .007), more extrathoracic (P < .001), and more multisite (P = .011) recurrences. Multivariable analysis of primary tumor factors revealed that, among patients who recurred, solid predominant histologic pattern in the primary tumor (hazard ratio [HR], 1.76; P = .016), age older than 65 years (HR, 1.63; P = .01), and sublobar resection (HR, 1.6; P = .01) were significantly associated with worse PRS. Presence of extrathoracic metastasis (HR, 1.76; P = .013) and age older than 65 years at the time of recurrence (HR, 1.7; P = .014) were also significantly associated with worse PRS.
Conclusion: In patients with stage I primary lung adenocarcinoma, solid predominant subtype is an independent predictor of early recurrence and, among those patients who recur, of worse PRS. Our findings provide a rationale for investigating adjuvant therapy and identify novel therapeutic targets for patients with solid predominant lung adenocarcinoma.
© 2015 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest are found in the article online at
Figures

References
-
- Martini N, Bains MS, Burt ME, et al. Incidence of local recurrence and second primary tumors in resected stage I lung cancer. J Thorac Cardiovasc Surg. 1995;109:120–129. - PubMed
-
- Goldstraw P, Crowley J, Chansky K, et al. The IASLC Lung Cancer Staging Project: Proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM Classification of malignant tumours. J Thorac Oncol. 2007;2:706–714. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
