

Prognostic significance of infarct core pathology revealed by quantitative non-contrast in comparison with contrast cardiac magnetic resonance imaging in reperfused ST-elevation myocardial infarction survivors
- PMID: 26261290
- PMCID: PMC4816961
- DOI: 10.1093/eurheartj/ehv372
Prognostic significance of infarct core pathology revealed by quantitative non-contrast in comparison with contrast cardiac magnetic resonance imaging in reperfused ST-elevation myocardial infarction survivors
Abstract
Aims: To assess the prognostic significance of infarct core tissue characteristics using cardiac magnetic resonance (CMR) imaging in survivors of acute ST-elevation myocardial infarction (STEMI).
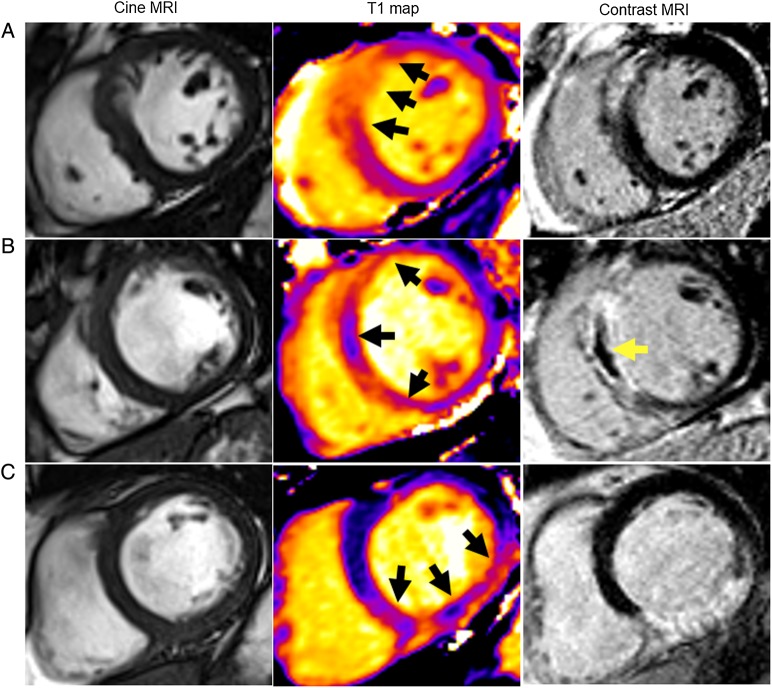
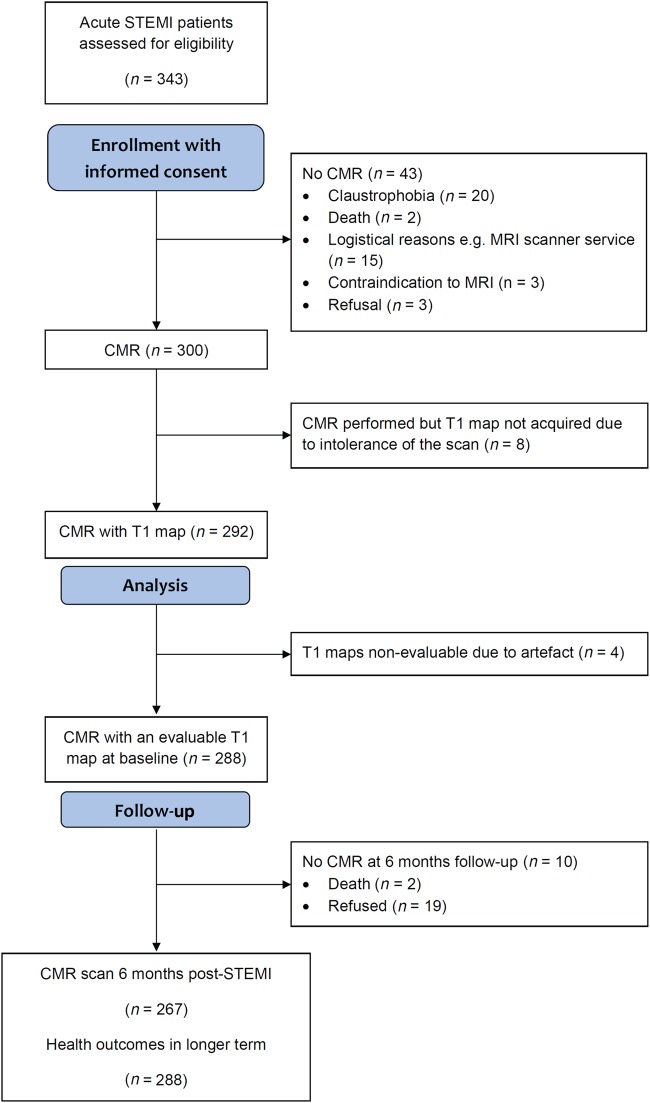
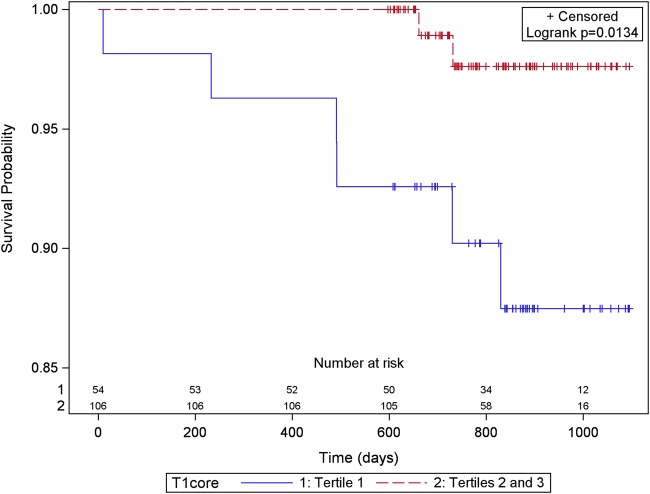
Methods and results: We performed an observational prospective single centre cohort study in 300 reperfused STEMI patients (mean ± SD age 59 ± 12 years, 74% male) who underwent CMR 2 days and 6 months post-myocardial infarction (n = 267). Native T1 was measured in myocardial regions of interest (n = 288). Adverse remodelling was defined as an increase in left ventricular (LV) end-diastolic volume ≥20% at 6 months. All-cause death or first heart failure hospitalization was a pre-specified outcome that was assessed during follow-up (median duration 845 days). One hundred and sixty (56%) patients had a hypo-intense infarct core disclosed by native T1. In multivariable regression, infarct core native T1 was inversely associated with adverse remodelling [odds ratio (95% confidence interval (CI)] per 10 ms reduction in native T1: 0.91 (0.82, 0.00); P = 0.061). Thirty (10.4%) of 288 patients died or experienced a heart failure event and 13 of these events occurred post-discharge. Native T1 values (ms) within the hypo-intense infarct core (n = 160 STEMI patients) were inversely associated with the risk of all-cause death or first hospitalization for heart failure post-discharge (for a 10 ms increase in native T1: hazard ratio 0.730, 95% CI 0.617, 0.863; P < 0.001) including after adjustment for left ventricular ejection fraction, infarct core T2 and myocardial haemorrhage. The prognostic results for microvascular obstruction were similar.
Conclusion: Infarct core native T1 represents a novel non-contrast CMR biomarker with potential for infarct characterization and prognostication in STEMI survivors. Confirmatory studies are warranted. CLINICALTRIALS.
Gov identifier: NCT02072850.
Keywords: Adverse remodelling; Cardiac magnetic resonance; Percutaneous coronary intervention; ST-elevation myocardial infarction.
© The Author 2015. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Risk stratification in acute myocardial infarction with multiparametric cardiac magnetic resonance imaging: getting to the core of the matter.Eur Heart J. 2016 Apr 1;37(13):1060-2. doi: 10.1093/eurheartj/ehv517. Epub 2015 Oct 20. Eur Heart J. 2016. PMID: 26486972 No abstract available.
References
-
- Holman BL, Chisholm RJ, Braunwald E. The prognostic implications of acute myocardial infarct scintigraphy with 99mTc-pyrophosphate. Circulation 1978;57:320–326. - PubMed
-
- Pfeffer MA, Braunwald E. Ventricular remodeling after myocardial infarction. Experimental observations and clinical implications. Circulation 1990;81:1161–1172. - PubMed
-
- van Kranenburg M, Magro M, Thiele H, de Waha S, Eitel I, Cochet A, Cottin Y, Atar D, Buser P, Wu E, Lee D, Bodi V, Klug G, Metzler B, Delewi R, Bernhardt P, Rottbauer W, Boersma E, Zijlstra F, van Geuns RJ. Prognostic value of microvascular obstruction and infarct size, as measured by CMR in STEMI patients. JACC Cardiovasc Imaging 2014;7:930–939. - PubMed
-
- Eitel I, Desch S, Fuernau G, Hildebrand L, Gutberlet M, Schuler G, Thiele H. Prognostic significance and determinants of myocardial salvage assessed by cardiovascular magnetic resonance in acute reperfused myocardial infarction. J Am Coll Cardiol 2010;55:2470–2479. - PubMed
-
- Eitel I, Kubusch K, Strohm O, Desch S, Mikami Y, de Waha S, Gutberlet M, Schuler G, Friedrich MG, Thiele H. Prognostic value and determinants of a hypointense infarct core in T2-weighted cardiac magnetic resonance in acute reperfused ST-elevation-myocardial infarction. Circ Cardiovasc Imaging 2011;4:354–362. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
