

Similar MR imaging characteristics but different pathological changes: a misdiagnosis for Lhermitte-Duclos disease and review of the literature
- PMID: 26261673
- PMCID: PMC4526007
Similar MR imaging characteristics but different pathological changes: a misdiagnosis for Lhermitte-Duclos disease and review of the literature
Abstract
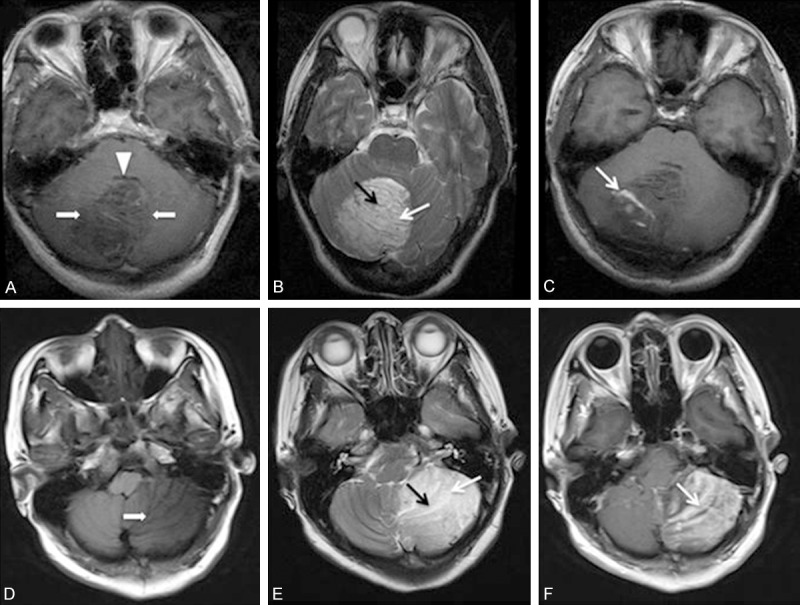
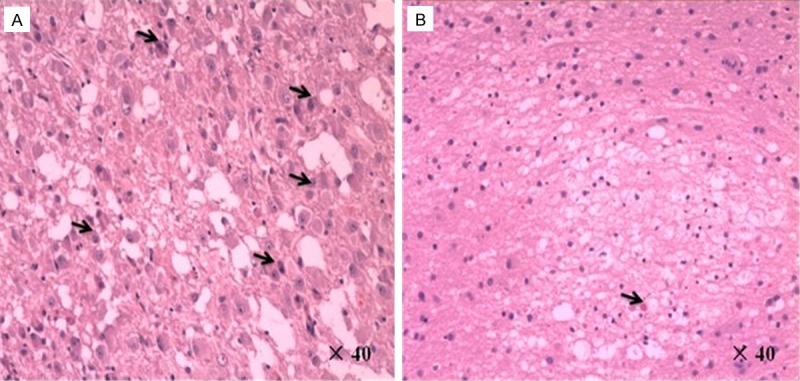
Although previous reports purpored that the unique magnetic resonance imaging (MRI) features of Lhermitte-Duclos disease (LDD) obviates the need for biopsy, we have made a misdiagnosis of LDD which has an indistinguishable imaging appearance. We present a patient who suffered from a normal cerebellum with arachnoid vascular malformation that had imaging characteristics which were indistinguishable from LDD before operation. This atypical imaging appearance, which could potentially be confused with LDD, may lead to misdiagnosis and inappropriate treatment in the absence of tissue sampling. Thus, this finding suggests that in those patients where images are highly suggestive of LDD but lack other manifestations of Cowden syndrome, biopsy is required and advanced imaging with magnetic resonance spectroscopy (MRS) should be strongly considered.
Keywords: Cowden syndrome; Lhermitte-Duclos disease; magnetic resonance imaging; misdiagnosis.
Figures
References
-
- Robinson S, Cohen AR. Cowden disease and Lhermitte-Duclos disease: characterization of a new phakomatosis. Neurosurgery. 2000;46:371–383. - PubMed
-
- Nowak DA, Trost HA, Porr A, Stolzle A, Lumenta CB. Lhermitte-Duclos disease (Dysplastic gangliocytoma of the cerebellum) Clin Neurol Neurosurg. 2001;103:105–110. - PubMed
-
- Thomas B, Krishnamoorthy T, Radhakrishnan VV, Kesavadas C. Advanced MR imaging in Lhermitte-Duclos disease: moving closer to pathology and pathophysiology. Neuroradiology. 2007;49:733–738. - PubMed
-
- Nowak DA, Trost HA. Lhermitte-Duclos disease (dysplastic cerebellar gangliocytoma): a malformation, hamartoma or neoplasm? Acta Neurol Scand. 2002;105:137–145. - PubMed
-
- Afshar-Oromieh A, Linhart H, Podlesek D, Schrempf W, Schackert G, Krex D. Postoperative cerebellar mutism in adult patients with Lhermitte-Duclos disease. Neurosurg Rev. 2010;33:401–408. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical