

Pancreatic adenocarcinoma pathology: changing "landscape"
- PMID: 26261723
- PMCID: PMC4502163
- DOI: 10.3978/j.issn.2078-6891.2015.032
Pancreatic adenocarcinoma pathology: changing "landscape"
Abstract
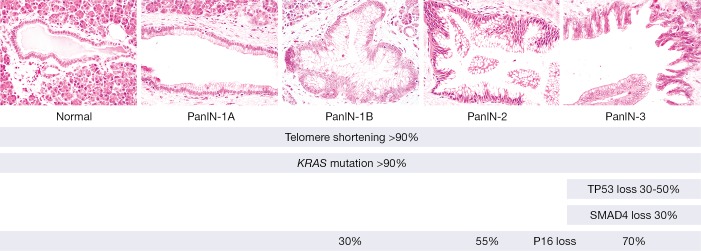
Pancreatic cancer is a devastating disease. At time of diagnosis the disease is usually advanced and only a minority of patients are eligible for surgical resection. The overall 5-year survival is 6%. However, survival of patients with early stage pancreatic cancer is significantly better. To improve the prognosis of patients with pancreatic cancer, it is essential to diagnose and treat pancreatic cancer in the earliest stage. Prevention of pancreatic cancer by treating noninvasive precursor lesions just before they invade tissues can potentially lead to even better outcomes. Pancreatic carcinogenesis results from a stepwise progression in which accumulating genetic alterations drive neoplastic progression in well-defined precursor lesions, ultimately giving rise to an invasive adenocarcinoma. A thorough understanding of the genetic changes that drive pancreatic carcinogenesis can lead to identification of biomarkers for early detection and targets for therapy. Recent next-generation sequencing (NGS) studies have shed new light on our understanding of the natural history of pancreatic cancer and the precursor lesions that give rise to these cancers. Importantly, there is a significant window of opportunity for early detection and treatment between the first genetic alteration in a cell in the pancreas and development of full-blown pancreatic cancer. The current views on the pathology and genetics of pancreatic carcinogenesis that evolved from studies of pancreatic cancer and its precursor lesions are discussed in this review.
Keywords: Pancreatic cancer; genetics; intraductal papillary mucinous neoplasm (IPMN); pancreatic intraepithelial neoplasia (PanIN); precursor lesions.
Figures
Similar articles
-
Precursor lesions of pancreatic cancer: molecular pathology and clinical implications.Pancreatology. 2007;7(1):9-19. doi: 10.1159/000101873. Epub 2007 Apr 18. Pancreatology. 2007. PMID: 17449961 Review.
-
Molecular mechanism of intraductal papillary mucinous neoplasm and intraductal papillary mucinous neoplasm-derived pancreatic ductal adenocarcinoma.J Hepatobiliary Pancreat Sci. 2015 Jul;22(7):519-23. doi: 10.1002/jhbp.246. Epub 2015 Apr 21. J Hepatobiliary Pancreat Sci. 2015. PMID: 25900667 Review.
-
Pancreatic intraepithelial neoplasia-can we detect early pancreatic cancer?Histopathology. 2010 Oct;57(4):503-14. doi: 10.1111/j.1365-2559.2010.03610.x. Epub 2010 Sep 28. Histopathology. 2010. PMID: 20875068 Review.
-
[Intraepithelial neoplasms (PanIN) and intraductal papillary-mucinous neoplasms (IPMN) of the pancreas as precursor lesions of pancreatic carcinoma].Med Klin (Munich). 2007 Feb 15;102(2):127-35. doi: 10.1007/s00063-007-1013-8. Med Klin (Munich). 2007. PMID: 17323019 Review. German.
-
Serine protease inhibitor Kazal type 1 and epidermal growth factor receptor are expressed in pancreatic tubular adenocarcinoma, intraductal papillary mucinous neoplasm, and pancreatic intraepithelial neoplasia.J Hepatobiliary Pancreat Sci. 2013 Aug;20(6):620-7. doi: 10.1007/s00534-012-0587-6. J Hepatobiliary Pancreat Sci. 2013. PMID: 23475261
Cited by
-
Aberrant NFATc1 signaling counteracts TGFβ-mediated growth arrest and apoptosis induction in pancreatic cancer progression.Cell Death Dis. 2019 Jun 6;10(6):446. doi: 10.1038/s41419-019-1682-2. Cell Death Dis. 2019. PMID: 31171768 Free PMC article.
-
MicroRNA in pancreatic ductal adenocarcinoma and its precursor lesions.World J Gastrointest Oncol. 2016 Jan 15;8(1):18-29. doi: 10.4251/wjgo.v8.i1.18. World J Gastrointest Oncol. 2016. PMID: 26798434 Free PMC article. Review.
-
Endoscopic Ultrasonography is a Promising Tool for Preoperative Prediction of the Operability of Pancreatic Carcinoma.J Gastrointest Cancer. 2022 Mar;53(1):197-203. doi: 10.1007/s12029-020-00567-w. Epub 2021 Jan 7. J Gastrointest Cancer. 2022. PMID: 33411255
-
Usefulness of Deep Learning Analysis for the Diagnosis of Malignancy in Intraductal Papillary Mucinous Neoplasms of the Pancreas.Clin Transl Gastroenterol. 2019 May 22;10(5):1-8. doi: 10.14309/ctg.0000000000000045. Clin Transl Gastroenterol. 2019. PMID: 31117111 Free PMC article.
-
Selective epigenetic alterations in RNF43 in pancreatic exocrine cells from high-fat-diet-induced obese mice; implications for pancreatic cancer.BMC Res Notes. 2024 Apr 15;17(1):106. doi: 10.1186/s13104-024-06757-0. BMC Res Notes. 2024. PMID: 38622664 Free PMC article.
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources