

Robotic pancreaticoduodenectomy for pancreatic adenocarcinoma: role in 2014 and beyond
- PMID: 26261726
- PMCID: PMC4502160
- DOI: 10.3978/j.issn.2078-6891.2015.027
Robotic pancreaticoduodenectomy for pancreatic adenocarcinoma: role in 2014 and beyond
Abstract
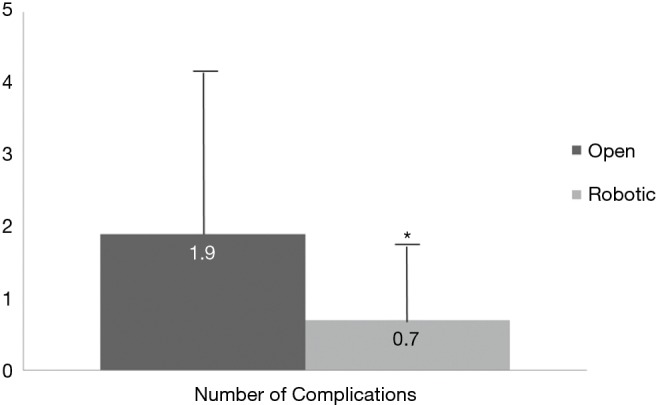
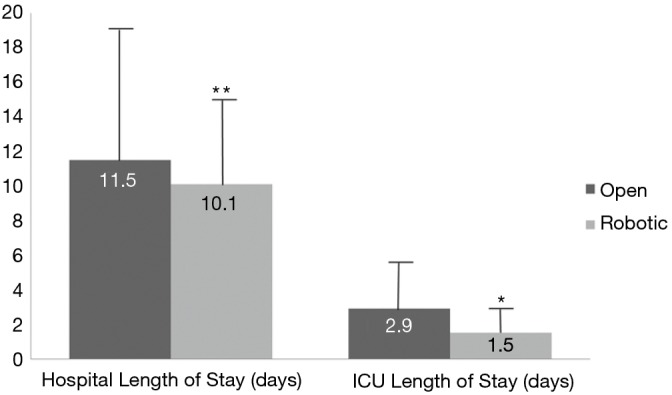
Minimally invasive surgery (MIS) for pancreatic adenocarcinoma has found new avenues for performing pancreaticoduodenectomy (PD) procedures, a historically technically challenging operation. Multiple studies have found laparoscopic PD to be safe, with equivalent oncologic outcomes as compared to open PD. In addition, several series have described potential benefits to minimally invasive PD including fewer postoperative complications, shorter hospital length of stay, and decreased postoperative pain. Yet, despite these promising initial results, laparoscopic PDs have not become widely adopted by the surgical community. In fact, the vast majority of pancreatic resections performed in the United States are still performed in an open fashion, and there are only a handful of surgeons who actually perform purely laparoscopic PDs. On the other hand, robotic assisted surgery offers many technical advantages over laparoscopic surgery including high-definition, 3-D optics, enhanced suturing ability, and more degrees of freedom of movement by means of fully-wristed instruments. Similar to laparoscopic PD, there are now several case series that have demonstrated the feasibility and safety of robotic PD with seemingly equivalent short-term oncologic outcomes as compared to open technique. In addition, having the surgeon seated for the procedure with padded arm-rests, there is an ergonomic advantage of robotics over both open and laparoscopic approaches, where one has to stand up for prolonged periods of time. Future technologic innovations will likely focus on enhanced robotic capabilities to improve ease of use in the operating room. Last but not least, robotic assisted surgery training will continue to be a part of surgical education curriculum ensuring the increased use of this technology by future generations of surgeons.
Keywords: Whipple; innovation; minimally invasive surgery (MIS); operative technique; pancreatic adenocarcinoma.
Figures
Similar articles
-
Should all distal pancreatectomies be performed laparoscopically?Adv Surg. 2009;43:283-300. doi: 10.1016/j.yasu.2009.02.013. Adv Surg. 2009. PMID: 19845186 Review.
-
Robotic pancreaticoduodenectomy for pancreatic head cancer and periampullary lesions.Ann Gastroenterol Surg. 2021 Mar 28;5(5):589-596. doi: 10.1002/ags3.12457. eCollection 2021 Sep. Ann Gastroenterol Surg. 2021. PMID: 34585043 Free PMC article. Review.
-
Contemporary review of minimally invasive pancreaticoduodenectomy.World J Gastrointest Surg. 2016 Dec 27;8(12):784-791. doi: 10.4240/wjgs.v8.i12.784. World J Gastrointest Surg. 2016. PMID: 28070234 Free PMC article.
-
Robot-assisted Sistrunk's operation, total thyroidectomy, and neck dissection via a transaxillary and retroauricular (TARA) approach in papillary carcinoma arising in thyroglossal duct cyst and thyroid gland.Ann Surg Oncol. 2012 Dec;19(13):4259-61. doi: 10.1245/s10434-012-2674-y. Epub 2012 Oct 16. Ann Surg Oncol. 2012. PMID: 23070784
-
Robotic arm enhancement to accommodate improved efficiency and decreased resource utilization in complex minimally invasive surgical procedures.Stud Health Technol Inform. 1996;29:471-81. Stud Health Technol Inform. 1996. PMID: 10172847
Cited by
-
A comparative study of robotics and laparoscopic in minimally invasive pancreatoduodenectomy: A single-center experience.Front Oncol. 2022 Oct 5;12:960241. doi: 10.3389/fonc.2022.960241. eCollection 2022. Front Oncol. 2022. PMID: 36276160 Free PMC article.
-
Learning curves for robotic pancreatic surgery-from distal pancreatectomy to pancreaticoduodenectomy.Medicine (Baltimore). 2018 Nov;97(45):e13000. doi: 10.1097/MD.0000000000013000. Medicine (Baltimore). 2018. PMID: 30407289 Free PMC article.
-
Internal Hernia Following Robotic Assisted Pancreaticoduodenectomy.Med Sci Monit. 2018 Apr 16;24:2287-2293. doi: 10.12659/msm.909273. Med Sci Monit. 2018. PMID: 29658495 Free PMC article.
-
Robotic versus open pancreatoduodenectomy for periampullary neoplasm: a propensity matched analysis of peri-operative and oncologic outcomes.Surg Endosc. 2025 Feb;39(2):922-931. doi: 10.1007/s00464-024-11423-4. Epub 2024 Dec 4. Surg Endosc. 2025. PMID: 39630267
-
Fast-Track Pancreaticoduodenectomy: Factors Associated with Early Discharge.World J Surg. 2019 May;43(5):1332-1341. doi: 10.1007/s00268-019-04916-0. World J Surg. 2019. PMID: 30680502
References
-
- Winer J, Can MF, Bartlett DL, et al. The current state of robotic-assisted pancreatic surgery. Nat Rev Gastroenterol Hepatol 2012;9:468-76. - PubMed
-
- Enomoto LM, Gusani NJ, Dillon PW, et al. Impact of surgeon and hospital volume on mortality, length of stay, and cost of pancreaticoduodenectomy. J Gastrointest Surg 2014;18:690-700. - PubMed
-
- Swan RZ, Niemeyer DJ, Seshadri RM, et al. The impact of regionalization of pancreaticoduodenectomy for pancreatic Cancer in North Carolina since 2004. Am Surg 2014;80:561-6. - PubMed
-
- Mesleh MG, Stauffer JA, Asbun HJ. Minimally invasive surgical techniques for pancreatic cancer: ready for prime time? J Hepatobiliary Pancreat Sci 2013;20:578-82. - PubMed
-
- Gagner M, Pomp A. Laparoscopic pylorus-preserving pancreatoduodenectomy. Surg Endosc 1994;8:408-10. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous