

From bronchiolitis guideline to practice: A critical care perspective
- PMID: 26261767
- PMCID: PMC4524812
- DOI: 10.5492/wjccm.v4.i3.152
From bronchiolitis guideline to practice: A critical care perspective
Abstract
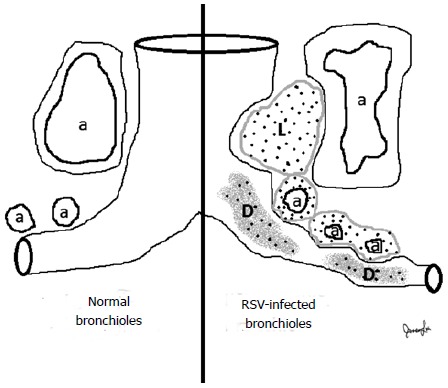
Acute viral bronchiolitis is a leading cause of admission to pediatric intensive care units, but research on the care of these critically ill infants has been limited. Pathology of viral bronchiolitis revealed respiratory obstruction due to intraluminal debris and edema of the airways and vasculature. This and clinical evidence suggest that airway clearance interventions such as hypertonic saline nebulizers and pulmonary toilet devices may be of benefit, particularly in situations of atelectasis associated with bronchiolitis. Research to distinguish an underlying asthma predisposition in wheezing infants with viral bronchiolitis may one day lead to guidance on when to trial bronchodilator therapy. Considering the paucity of critical care research in pediatric viral bronchiolitis, intensive care practitioners must substantially rely on individualization of therapies based on bedside clinical assessments. However, with the introduction of new diagnostic and respiratory technologies, our ability to support critically ill infants with acute viral bronchiolitis will continue to advance.
Keywords: Acute viral bronchiolitis; Asthma; Hypertonic nebulized saline; Respiratory syncytial virus; Rhinovirus.
Figures
References
-
- Prais D, Schonfeld T, Amir J. Admission to the intensive care unit for respiratory syncytial virus bronchiolitis: a national survey before palivizumab use. Pediatrics. 2003;112:548–552. - PubMed
-
- Prodhan P, Sharoor-Karni S, Lin J, Noviski N. Predictors of respiratory failure among previously healthy children with respiratory syncytial virus infection. Am J Emerg Med. 2011;29:168–173. - PubMed
-
- Blumenthal D, Tavenner M. The “meaningful use” regulation for electronic health records. N Engl J Med. 2010;363:501–504. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
