

Binocular versus standard occlusion or blurring treatment for unilateral amblyopia in children aged three to eight years
- PMID: 26263202
- PMCID: PMC6718221
- DOI: 10.1002/14651858.CD011347.pub2
Binocular versus standard occlusion or blurring treatment for unilateral amblyopia in children aged three to eight years
Update in
-
Binocular versus standard occlusion or blurring treatment for unilateral amblyopia in children aged three to eight years.Cochrane Database Syst Rev. 2022 Feb 7;2(2):CD011347. doi: 10.1002/14651858.CD011347.pub3. Cochrane Database Syst Rev. 2022. PMID: 35129211 Free PMC article.
Abstract
Background: Current treatments for amblyopia in children, occlusion and pharmacological blurring, have had limited success, with less than two-thirds of children achieving good visual acuity of at least 0.20 logMAR in the amblyopic eye, limited improvement of stereopsis, and poor compliance. A new treatment approach, based on the dichoptic presentation of movies or computer games (images presented separately to each eye), may yield better results, as it aims to balance the input of visual information from each eye to the brain. Compliance may also improve with these more child-friendly treatment procedures.
Objectives: To determine whether binocular treatments in children aged three to eight years with unilateral amblyopia result in better visual outcomes than conventional occlusion or pharmacological blurring treatment.
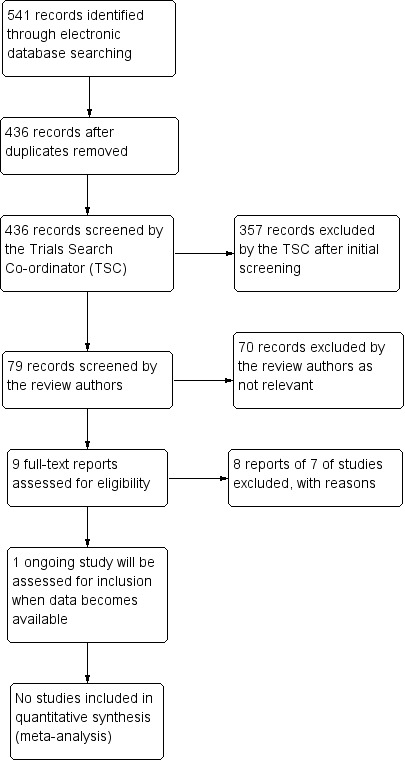
Search methods: We searched the Cochrane Eyes and Vision Group Trials Register (last date of searches: 14 April 2015), the Cochrane Central Register of Controlled Trials (CENTRAL; 2015, Issue 3), Ovid MEDLINE, Ovid MEDLINE In-Process and Other Non-Indexed Citations, Ovid MEDLINE Daily, Ovid OLDMEDLINE (January 1946 to April 2015), EMBASE (January 1980 to April 2015), the ISRCTN registry (www.isrctn.com/editAdvancedSearch), ClinicalTrials.gov (www.clinicaltrials.gov), and the World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) (www.who.int/ictrp/search/en). We did not use any date or language restrictions in the electronic searches for trials.
Selection criteria: Two review authors independently screened the results of the search in order to identify studies that met the inclusion criteria of the review: randomised controlled trials (RCTs) that enrolled participants between the ages of three and eight years old with unilateral amblyopia, defined as best-corrected visual acuity (BCVA) worse than 0.200 logMAR in the amblyopic eye, and BCVA 0.200 logMAR or better in the fellow eye, in the presence of an amblyogenic risk factor such as anisometropia, strabismus, or both. Prior to enrolment, participants were to have undergone a cycloplegic refraction and comprehensive ophthalmic examination including fundal examination. In addition, participants had to have completed a period of optical treatment, if indicated, and BCVA in the amblyopic eye had to remain unchanged on two consecutive assessments despite reportedly good compliance with glasses wearing. Participants were not to have received any treatment other than optical treatment prior to enrolment. We planned to include any type of binocular viewing intervention; these could be delivered on different devices including computer monitors viewed with LCD shutter glasses or hand-held screens including mobile phone screens with lenticular prism overlay. Control groups were to have received standard amblyopia treatment; this could include occlusion or pharmacological blurring of the better-seeing eye. We planned to include full-time (all waking hours) and part-time (between 1 and 12 hours a day) occlusion regimens.
Data collection and analysis: We planned to use standard methodological procedures expected by The Cochrane Collaboration. We had planned to meta-analyse the primary outcome, that is mean distance BCVA in the amblyopic eye at 12 months after the cessation of treatment.
Main results: We could identify no RCTs in this subject area.
Authors' conclusions: Further research is required to allow decisions about implementation of binocular treatments for amblyopia in clinical practice. Currently there are no clinical trials offering standardised evidence of the safety and effectiveness of binocular treatments, but results from non-controlled cohort studies are encouraging. Future research should be conducted in the form of RCTs, using acknowledged methods of visual acuity and stereoacuity assessment with known reproducibility. Other important outcome measures include outcomes reported by users, compliance with treatment, and recurrence of amblyopia after cessation of treatment.
Conflict of interest statement
No financial interests to declare.
Figures
References
References to studies excluded from this review
-
- Bau V, Rose K, Pollack K, Spoerl E, Pillunat LE. Effectivity of an occlusion‐supporting PC‐based visual training programme by horizontal drifting sinus gratings in children with amblyopia. Klinische Monatsblatter fur Augenheilkunde 2012;229(10):979‐86. - PubMed
-
- Chen PL, Chen JT, Fu JJ, Chien KH, Lu DW. A pilot study of anisometropic amblyopia improved in adults and children by perceptual learning: an alternative treatment to patching. Ophthalmic and Physiological Optics 2008;28(5):422‐8. - PubMed
-
- Foss AJ, Gregson RM, MacKeith D, Herbison N, Ash IM, Cobb SV, et al. Evaluation and development of a novel binocular treatment (I‐BiT) system using video clips and interactive games to improve vision in children with amblyopia ('lazy eye'): study protocol for a randomised controlled trial. Trials 2013;14:145. - PMC - PubMed
- NCT01702727. Evaluation and development of a novel binocular treatment (I‐BiTTM) system using video clips and interactive games to improve vision in children with amblyopia ('lazy eye'). clinicaltrials.gov/ct2/show/NCT01702727 (accessed 20 November 2014). - PMC - PubMed
References to ongoing studies
-
- NCT02200211. Study of binocular computer activities for treatment of amblyopia. clinicaltrials.gov/ct2/show/NCT02200211 (accessed 10 October 2014).
Additional references
-
- Awan M, Proudlock FA, Gottlob I. A randomized controlled trial of unilateral strabismic and mixed amblyopia using occlusion dose monitors to record compliance. Investigative Ophthalmology and Visual Science 2005;46(4):1435‐9. - PubMed
References to other published versions of this review
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous