

Systematic review of enhanced recovery after gastro-oesophageal cancer surgery
- PMID: 26263799
- PMCID: PMC4474007
- DOI: 10.1308/003588414X14055925061630
Systematic review of enhanced recovery after gastro-oesophageal cancer surgery
Abstract
Introduction: Fast track methodology or enhanced recovery schemes have gained increasing popularity in perioperative care. While evidence is strong for colorectal surgery, its importance in gastric and oesophageal surgery has yet to be established. This article reviews the evidence of enhanced recovery schemes on outcome for this type of surgery.
Methods: A systematic literature search was conducted up to March 2014. Studies were retrieved and analysed using predetermined criteria.
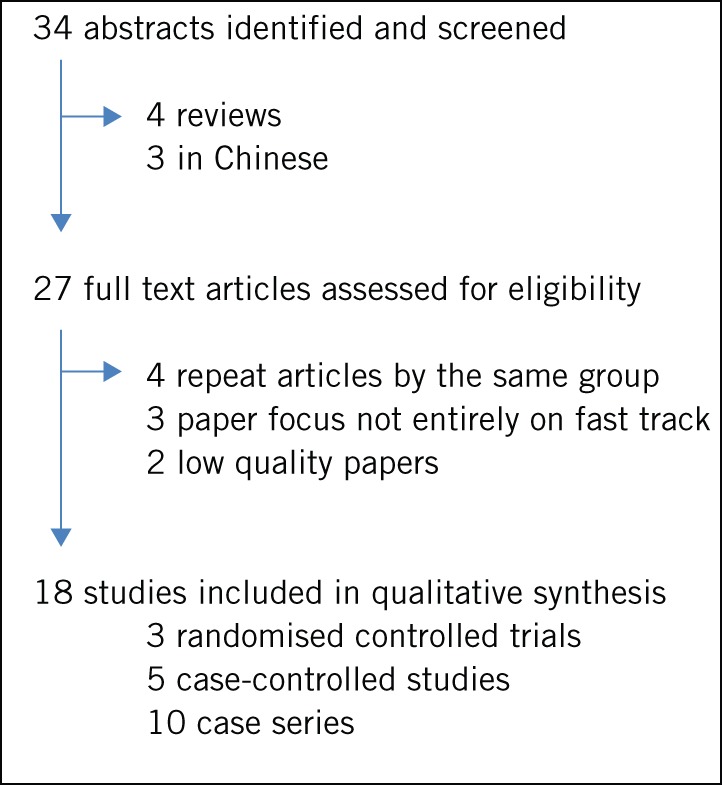
Results: From 34 articles reviewed, 18 eligible studies were identified: 7 on gastric and 11 on oesophageal resection. Three randomised controlled trials, five case-controlled studies and ten case series were identified. The reported protocols included changes to each stage of the patient journey from pre to postoperative care. The specific focus following oesophageal resections was on early mobilisation, a reduction in intensive care unit stay, early drain removal and early (or no) contrast swallow studies. Following gastric resections, the emphasis was on reducing epidural anaesthesia along with re-establishing oral intake in the first three postoperative days and early removal of nasogastric tubes. In the papers reviewed, mortality rates following fast track surgery were 0.8% (9/1,075) for oesophageal resection and 0% (0/329) for gastric resection. The reported morbidity rate was 16.5% (54/329) following gastric resection and 38.6% (396/1,075) following oesophageal resection. Length of stay was reduced in both groups compared with conventional recovery groups in comparative studies.
Conclusions: The evidence for enhanced recovery schemes following gastric and oesophageal resection is weak, with only three (low volume) published randomised controlled trials. However, the enhanced recovery approach appears safe and may be associated with a reduction in length of stay.
Keywords: Enhanced recovery; Gastrectomy; Oesophagectomy.
References
-
- National Oesophago-Gastric Cancer Audit 2013. London: RCS; 2013.
-
- Blazeby JM, Farndon JR, Donovan J, Alderson D. A prospective longitudinal study examining the quality of life of patients with esophageal carcinoma. Cancer 2000; 88: 1,781–1,787. - PubMed
-
- Kehlet H, Wilmore DW. Multimodal strategies to improve surgical outcome. Am J Surg 2002; 183: 630–641. - PubMed
-
- Kehlet H, Dahl JB. Anaesthesia, surgery, and challenges in postoperative recovery. Lancet 2003; 362: 1,921–1,928. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical