

Ossifying metaplasia of urothelial metastases: original case with review of the literature
- PMID: 26264044
- PMCID: PMC4534062
- DOI: 10.1186/s12880-015-0072-1
Ossifying metaplasia of urothelial metastases: original case with review of the literature
Abstract
Background: Ossifying metaplasia is an unusual feature of urothelial carcinoma, with only a few cases reported. The largest series included 17 cases and was published in 1991. The mechanism of ossification is unknown and hypotheses of osteogenic precursor cells, inducing bone formation, are proposed.
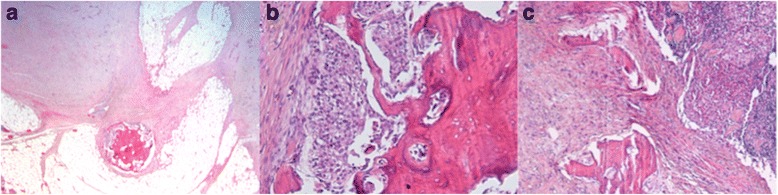
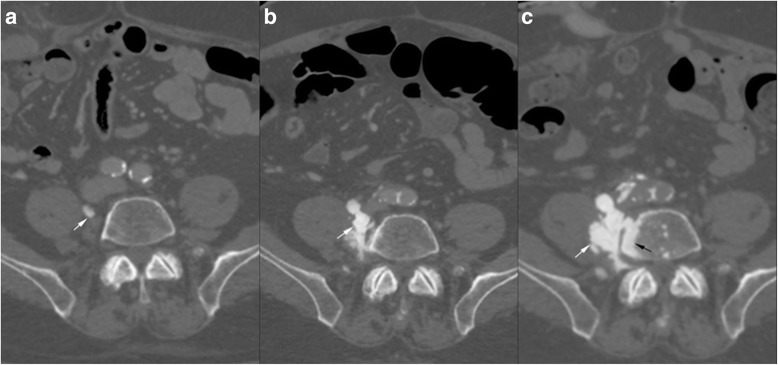
Case presentation: A 75 year-old patient was treated for a high grade transitional cell carcinoma of the bladder by surgery, chemotherapy and radiotherapy. Histology showed foci of bone metaplasia, both at the periphery of the tumor, and in a lymph node metastasis. 1 year later, a heterotopic bone formation was discovered in the right retroperitoneal space, near the lumbar spine, increasing rapidly in size during follow-up. Several imaging exams were performed (2 CT, 1 MRI, 1 Pet-CT), but in the absence of typical features of sarcoma, diagnosis remained unclear. Histology of a CT-guided percutaneous biopsy showed urothelial carcinoma and mature lamellar bone. Integration of these findings with the radiological description of extraosseous localization was consistent with a diagnosis of osseous metaplasia of an urothelial carcinoma metastasis. The absence of bone atypia in both the primary and metastases argues against sarcomatoid urothelial carcinoma with osteosarcomatous differentiation.
Conclusion: Osseous metaplasia of an urothelial carcinoma metastasis is unusual, and difficult to distinguish from radiotherapy induced sarcoma, or from sarcomatoid carcinoma. Rapid progression, sheathing of adjacent structures such as vessels (like inferior vena cava in our case) and nerves and bony feature of lymph node metastases necessitate histological confirmation and rapid treatment. Our case illustrates this disease and evaluates the imaging features. In addition we discuss the differential diagnosis of osseous retroperitoneal masses.
Figures






References
-
- Cormio L, Sanguedolce F, Massenio P, Di Fino G, Selvaggio O, Bufo P, Carrieri G. Osseous metaplasia within a urothelial bladder cancer nodal metastasis: a case report. Anal Quant Cytopathol Histpathol. 2014;36(2):117–9. - PubMed
-
- Amin MB, Trpkov K, Lopez-Beltran A, Grignon D, Members of the ISUP Immunohistochemistry in Diagnostic Urologic Pathology Group Best practices recommendations in the application of immunohistochemistry in the bladder lesions: report from the International Society of Urologic Pathology consensus conference. Am J Surg Pathol. 2014;38(8):e20–34. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
