

Variable alterations of the microbiota, without metabolic or immunological change, following faecal microbiota transplantation in patients with chronic pouchitis
- PMID: 26264409
- PMCID: PMC4532993
- DOI: 10.1038/srep12955
Variable alterations of the microbiota, without metabolic or immunological change, following faecal microbiota transplantation in patients with chronic pouchitis
Abstract
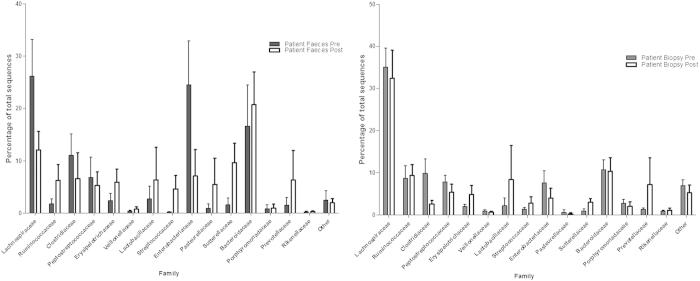
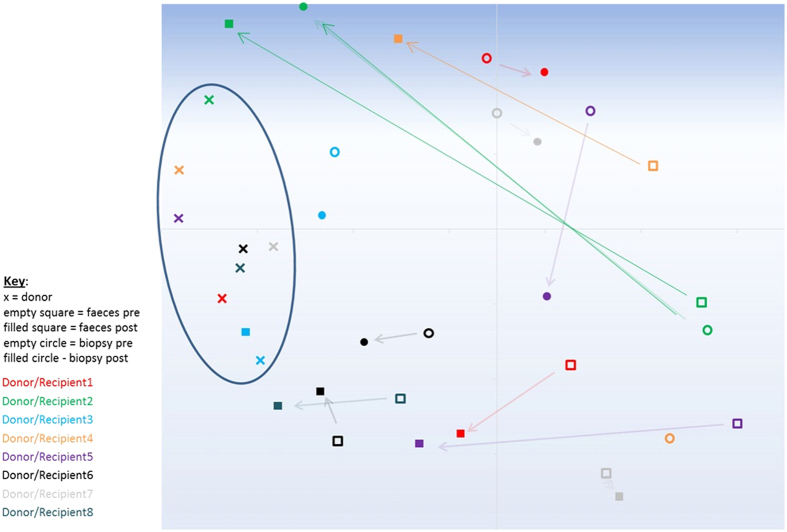
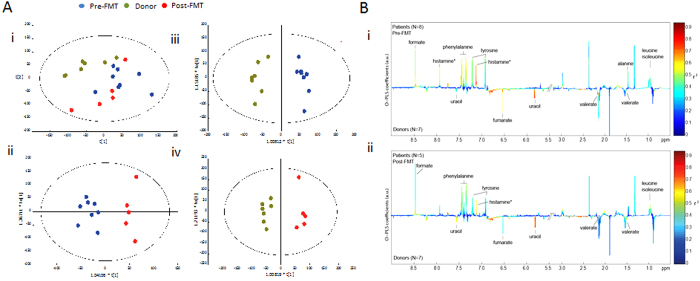
Faecal microbiota transplantation (FMT) is effective in the treatment of Clostridium difficile infection, where efficacy correlates with changes in microbiota diversity and composition. The effects of FMT on recipient microbiota in inflammatory bowel diseases (IBD) remain unclear. We assessed the effects of FMT on microbiota composition and function, mucosal immune response, and clinical outcome in patients with chronic pouchitis. Eight patients with chronic pouchitis (current PDAI ≥7) were treated with FMT via nasogastric administration. Clinical activity was assessed before and four weeks following FMT. Faecal coliform antibiotic sensitivities were analysed, and changes in pouch faecal and mucosal microbiota assessed by 16S rRNA gene pyrosequencing and (1)H NMR spectroscopy. Lamina propria dendritic cell phenotype and cytokine profiles were assessed by flow cytometric analysis and multiplex assay. Following FMT, there were variable shifts in faecal and mucosal microbiota composition and, in some patients, changes in proportional abundance of species suggestive of a "healthier" pouch microbiota. However, there were no significant FMT-induced metabolic or immunological changes, or beneficial clinical response. Given the lack of clinical response following FMT via a single nasogastric administration our results suggest that FMT/bacteriotherapy for pouchitis patients requires further optimisation.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
