

Socio-cultural factors, gender roles and religious ideologies contributing to Caesarian-section refusal in Nigeria
- PMID: 26265149
- PMCID: PMC4534149
- DOI: 10.1186/s12978-015-0050-7
Socio-cultural factors, gender roles and religious ideologies contributing to Caesarian-section refusal in Nigeria
Abstract
Background: The death of women from pregnancy-related causes is a serious challenge that international development initiatives, including the Millennium Development Goals, have been trying to redress for decades. The majority of these pregnancy-related deaths occur in developing countries especially in Sub-Saharan Africa. The provision of Emergency Obstetric Care (EmOC), including Caesarean section (CS) has been identified as one of the key ingredients necessary for the reduction of high maternal mortality ratios. However, it appears that creating access to EmOC facilities is not all that is required to reduce maternal mortality: socio-cultural issues in Sub-Saharan countries including Nigeria seem to deter women from accepting CS. This study seeks to explore some of the socio-cultural concerns that reinforce delays and non-acceptance of CS in a Nigerian community.
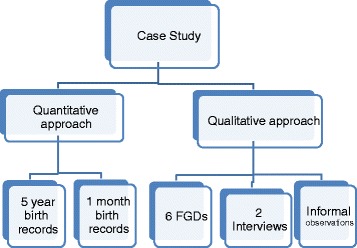
Methods: This is a mixed method study that combined both qualitative and quantitative strategies of enquiry. The hospital's delivery records from 2006-2010 provided data for quantitative analysis. This quantitative data was supplemented with prospective data collected during one month. Semi-structured interviews, focus group discussions (FGD) and informal observations served as the sources of data on the qualitative end.
Results: In total, 22% of maternity clients refused CS and more than 90% of the CSs in the focal hospital were emergencies which may indicate late arrival at the hospital after seeking assistance elsewhere. The qualitative analysis reveals that socio-cultural meanings informed by gender and religious ideologies, the relational consequences of having a C-section, and the role of alternative providers are some key factors which influence when, where and whether women will accept C-section or not.
Conclusion: There is need to find means of facilitating necessary CS by addressing the prevailing socio-cultural norms and expectations that hinder its acceptance. Engaging and guiding alternative providers (traditional birth attendants and faith healers) who wield much power in their communities, will be important to minimize delays and improve cultural acceptability of CS.
Figures
References
-
- WHO, UNICEF, UNFPA, World Bank . Trends in maternal mortality: 2013 estimates. Geneva: World Health Organization; 2014.
-
- UNICEF. WHO . Countdown to 2015. Fulfilling the Health Agenda for Women and Children: The 2014 Report. Geneva: UNICEF and WHO; 2014.
-
- United Nations. Report of the Open Working Group of the General Assembly on Sustainable Development Goals. 2014. http://www.un.org/ga/search/view_doc.asp?symbol=A/68/970&Lang=E. Accessed 24 April 2015.
-
- World Health Organisation. Monitoring Emergency Obstetric Care: a handbook. 2009. Accessed 13 February 2012.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
