

Chromosomal copy number alterations for associations of ductal carcinoma in situ with invasive breast cancer
- PMID: 26265211
- PMCID: PMC4534146
- DOI: 10.1186/s13058-015-0623-y
Chromosomal copy number alterations for associations of ductal carcinoma in situ with invasive breast cancer
Abstract
Introduction: Screening mammography has contributed to a significant increase in the diagnosis of ductal carcinoma in situ (DCIS), raising concerns about overdiagnosis and overtreatment. Building on prior observations from lineage evolution analysis, we examined whether measuring genomic features of DCIS would predict association with invasive breast carcinoma (IBC). The long-term goal is to enhance standard clinicopathologic measures of low- versus high-risk DCIS and to enable risk-appropriate treatment.
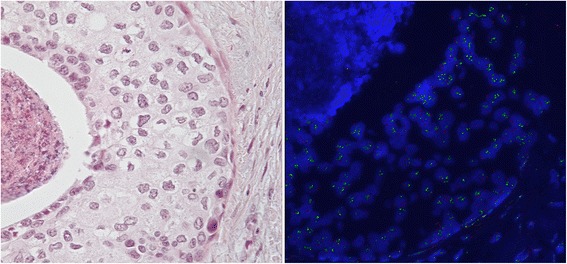
Methods: We studied three common chromosomal copy number alterations (CNA) in IBC and designed fluorescence in situ hybridization-based assay to measure copy number at these loci in DCIS samples. Clinicopathologic data were extracted from the electronic medical records of Stanford Cancer Institute and linked to demographic data from the population-based California Cancer Registry; results were integrated with data from tissue microarrays of specimens containing DCIS that did not develop IBC versus DCIS with concurrent IBC. Multivariable logistic regression analysis was performed to describe associations of CNAs with these two groups of DCIS.
Results: We examined 271 patients with DCIS (120 that did not develop IBC and 151 with concurrent IBC) for the presence of 1q, 8q24 and 11q13 copy number gains. Compared to DCIS-only patients, patients with concurrent IBC had higher frequencies of CNAs in their DCIS samples. On multivariable analysis with conventional clinicopathologic features, the copy number gains were significantly associated with concurrent IBC. The state of two of the three copy number gains in DCIS was associated with a risk of IBC that was 9.07 times that of no copy number gains, and the presence of gains at all three genomic loci in DCIS was associated with a more than 17-fold risk (P = 0.0013).
Conclusions: CNAs have the potential to improve the identification of high-risk DCIS, defined by presence of concurrent IBC. Expanding and validating this approach in both additional cross-sectional and longitudinal cohorts may enable improved risk stratification and risk-appropriate treatment in DCIS.
Figures

References
-
- Bleyer A, Welch HG. Effect of screening mammography on breast cancer incidence. N Engl J Med. 2013;368:679. - PubMed
-
- Ries L, Melbert D, Krapcho M. SEER cancer statistics review, 1975–2004. Bethesda, MD: National Cancer Institute; 2007.
-
- Clarke M, Collins R, Darby S, Davies C, Elphinstone P, Evans E, et al. Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;366:2087–106. doi: 10.1016/S0140-6736(05)67887-7. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
