

Bilateral periorbital and cervicofacial emphysema following retinal surgery and fluid gas exchange in a case of inadvertent globe perforation
- PMID: 26265649
- PMCID: PMC4550992
- DOI: 10.4103/0301-4738.162615
Bilateral periorbital and cervicofacial emphysema following retinal surgery and fluid gas exchange in a case of inadvertent globe perforation
Abstract
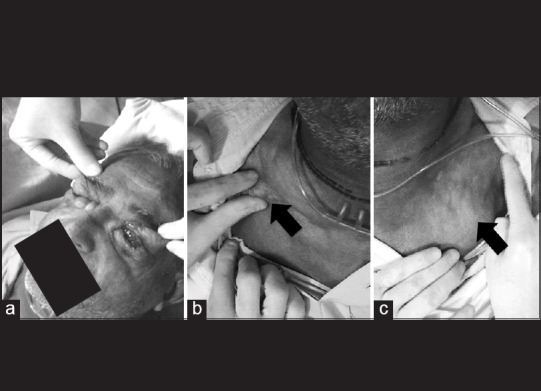
Surgical emphysema is defined as gas or air trapped in the subcutaneous tissue plane. Here, we report a rare case of bilateral periorbital and cervicofacial subcutaneous emphysema following a vitreoretinal surgery for inadvertent globe perforation during the administration of peribulbar anesthesia. This condition, although self-resolving when restricted to the subcutaneous plane has the potential to spread into deeper tissue planes such as the retropharyngeal space. The presence of crepitus helps to distinguish it from angioneurotic edema. Ophthalmologists must be sensitive to the fact that surgical emphysema can be a very rare, but possible complication of an intraocular surgery following globe perforation.
Conflict of interest statement
Figures

References
-
- Mather AJ, Stoykewych AA, Curran JB. Cervicofacial and mediastinal emphysema complicating a dental procedure. J Can Dent Assoc. 2006;72:565–8. - PubMed
-
- Fleischman D, Davis RM, Lee LB. Subcutaneous and periorbital emphysema following dental procedure. Ophthal Plast Reconstr Surg. 2014;30:e43–5. - PubMed
-
- Katz SE, Lubow M, Jacoby J. Suck and spit, don’t blow: Orbital emphysema after decompression surgery. Ophthalmology. 1999;106:1303–5. - PubMed
-
- Goldberg MH, Toazian RG. Oral and Maxillofacial Infections. 2nd ed. Philadelphia: WB Saunders Company; 1987. Odontogenic infections and deep fascial space infections of dental origin; p. 171.
-
- Ajit R, Inkster C, Tuck J, Mortzos P. Orbital emphysema: An unusual complication of balloon dacryocystoplasty. Br J Radiol. 2004;77:1057–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
