

Esophageal Perforation and Acute Bacterial Mediastinitis: Other Causes of Chest Pain That Can Be Easily Missed
- PMID: 26266352
- PMCID: PMC4616702
- DOI: 10.1097/MD.0000000000001232
Esophageal Perforation and Acute Bacterial Mediastinitis: Other Causes of Chest Pain That Can Be Easily Missed
Abstract
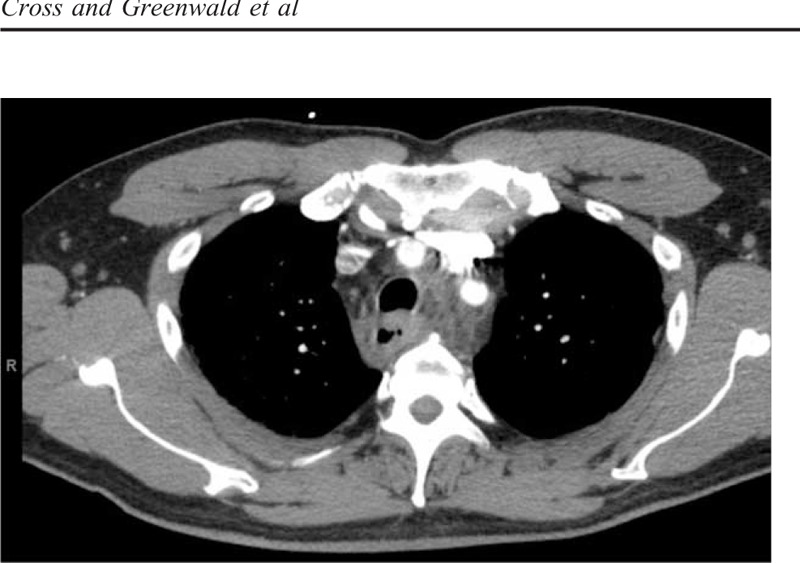
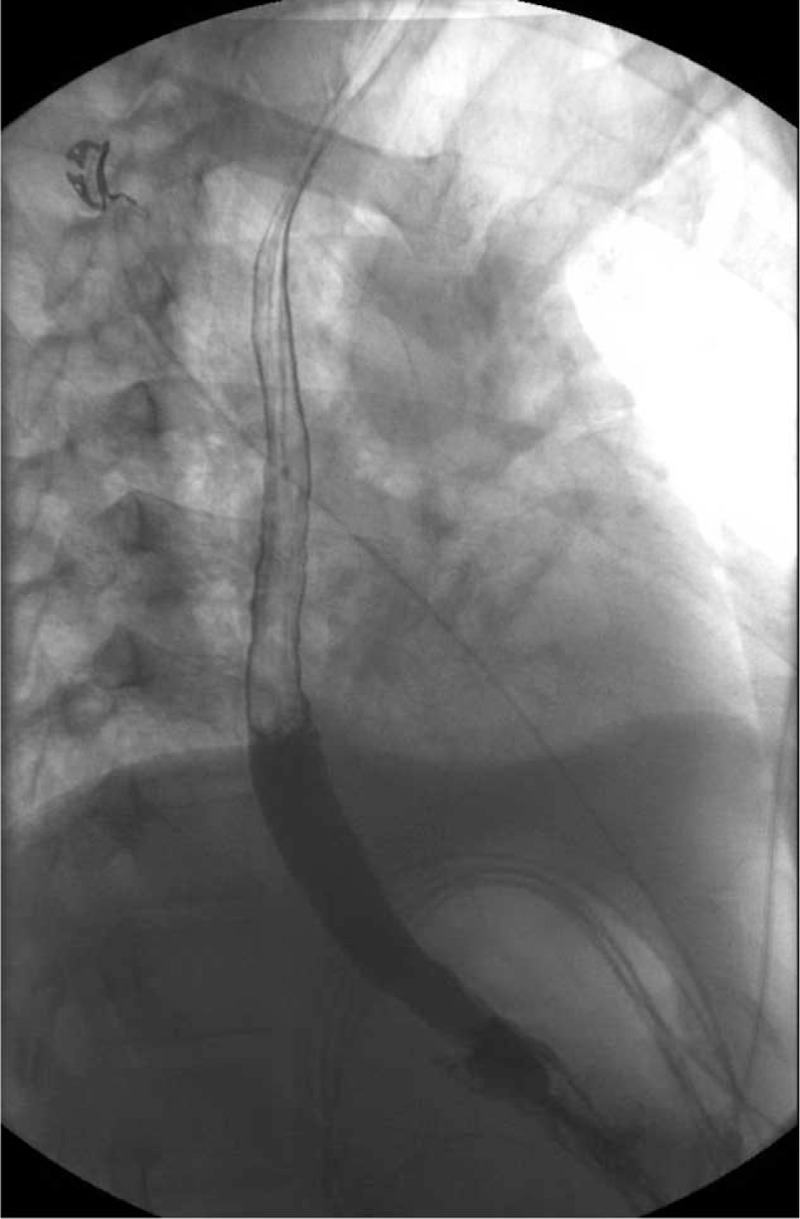
Esophageal perforation is a rare condition that is commonly missed. Male gender and alcohol use are predisposing risk factors. Most of the cases are iatrogenic or traumatic; nonetheless, spontaneous cases are not uncommon. It typically occurs after vomiting or straining as the increased intra-abdominal pressure transmits into the esophagus and results in the tear. One of the main complications is acute bacterial mediastinitis from contamination with esophageal flora. This condition can be life-threatening because it is very frequently misdiagnosed and appropriate management is often delayed.A 49-year-old man presented with worsening sudden-onset interscapular back pain that then changed to chest pain with odynophagia and was found to have fever and leukocytosis.Chest computed tomography revealed signs of mediastinitis with possible esophageal perforation. He reported symptoms started 2 days ago after lifting of heavy objects. Empiric antimicrobial was begun with conservative management and avoidance of oral intake. Barium esophagram and esophagogastroduodenoscopy revealed no signs of perforation or inflammation. His symptoms resolved and he gradually resumed oral intake. Blood cultures grew Methicillin-sensitive Staphylococcus aureus and he was discharged on appropriate antibiotics for 4 weeks. He did well on follow-up 3 months after hospitalization.The case highlights the importance of considering esophageal etiologies of chest pain.
Figures
References
-
- Vidarsdottir H, Blondal S, Alfredsson H, et al. Oesophageal perforations in Iceland: a whole population study on incidence, aetiology and surgical outcome. Thorac Cardiovasc Surg 2010; 58:476–480. - PubMed
-
- Brinster CJ, Singhal S, Lee L, et al. Evolving options in the management of esophageal perforation. Ann Thorac Surg 2004; 77:1475–1483. - PubMed
-
- Clément R1, Bresson C, Rodat O. Spontaneous oesophageal perforation. J Clin Forensic Med 2006; 13:353–355. - PubMed
-
- Brauer RB, Liebermann-Meffert D, Stein HJ, et al. Boerhaave's syndrome: analysis of the literature and report of 18 new cases. Dis Esophagus 1997; 10:64–68. - PubMed
-
- Bladergroen MR, Lowe JE, Postlethwait RW. Diagnosis and recommended management of esophageal perforation and rupture. Ann Thorac Surg 1986; 42:235. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
