

Association of Thalamic Dysconnectivity and Conversion to Psychosis in Youth and Young Adults at Elevated Clinical Risk
- PMID: 26267151
- PMCID: PMC4892891
- DOI: 10.1001/jamapsychiatry.2015.0566
Association of Thalamic Dysconnectivity and Conversion to Psychosis in Youth and Young Adults at Elevated Clinical Risk
Abstract
Importance: Severe neuropsychiatric conditions, such as schizophrenia, affect distributed neural computations. One candidate system profoundly altered in chronic schizophrenia involves the thalamocortical networks. It is widely acknowledged that schizophrenia is a neurodevelopmental disorder that likely affects the brain before onset of clinical symptoms. However, no investigation has tested whether thalamocortical connectivity is altered in individuals at risk for psychosis or whether this pattern is more severe in individuals who later develop full-blown illness.
Objectives: To determine whether baseline thalamocortical connectivity differs between individuals at clinical high risk for psychosis and healthy controls, whether this pattern is more severe in those who later convert to full-blown illness, and whether magnitude of thalamocortical dysconnectivity is associated with baseline prodromal symptom severity.
Design, setting, and participants: In this multicenter, 2-year follow-up, case-control study, we examined 397 participants aged 12-35 years of age (243 individuals at clinical high risk of psychosis, of whom 21 converted to full-blown illness, and 154 healthy controls). The baseline scan dates were January 15, 2010, to April 30, 2012.
Main outcomes and measures: Whole-brain thalamic functional connectivity maps were generated using individuals' anatomically defined thalamic seeds, measured using resting-state functional connectivity magnetic resonance imaging.
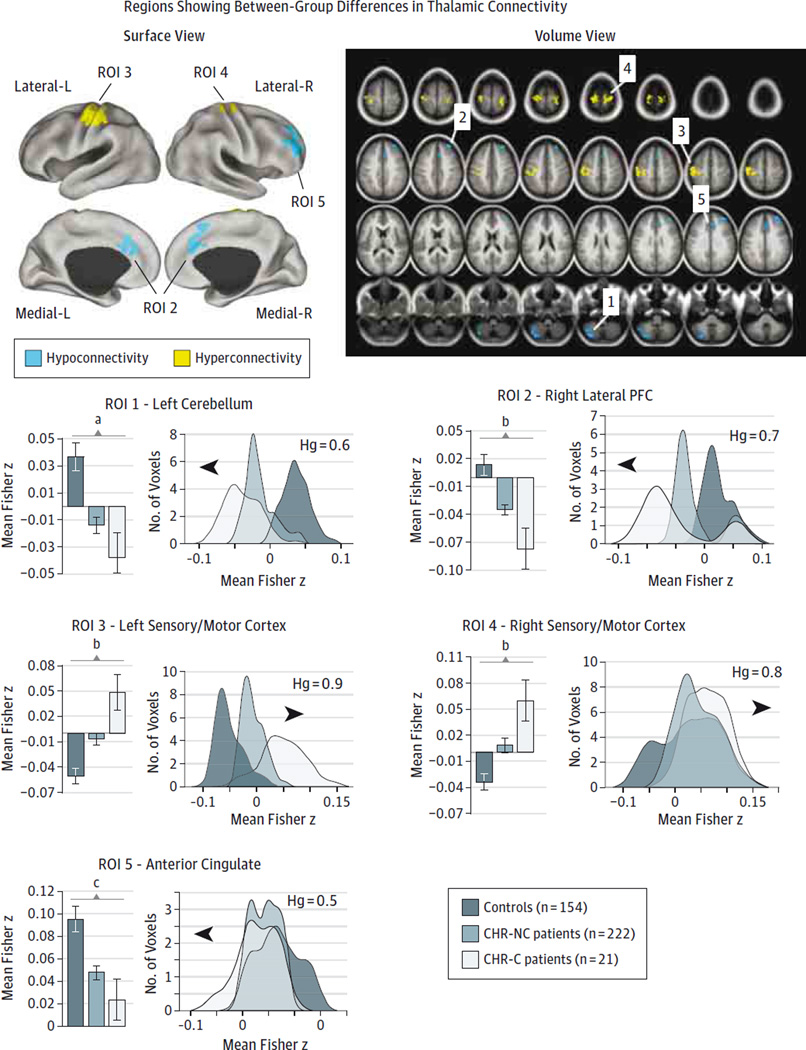
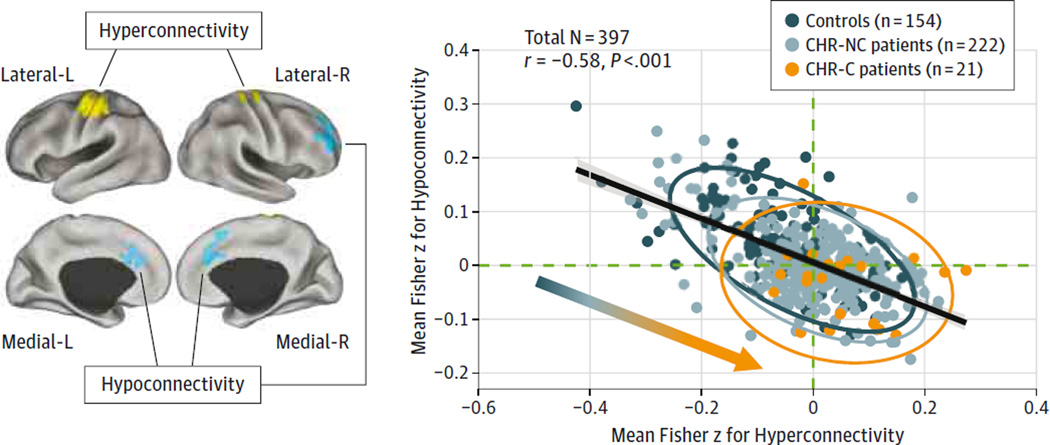
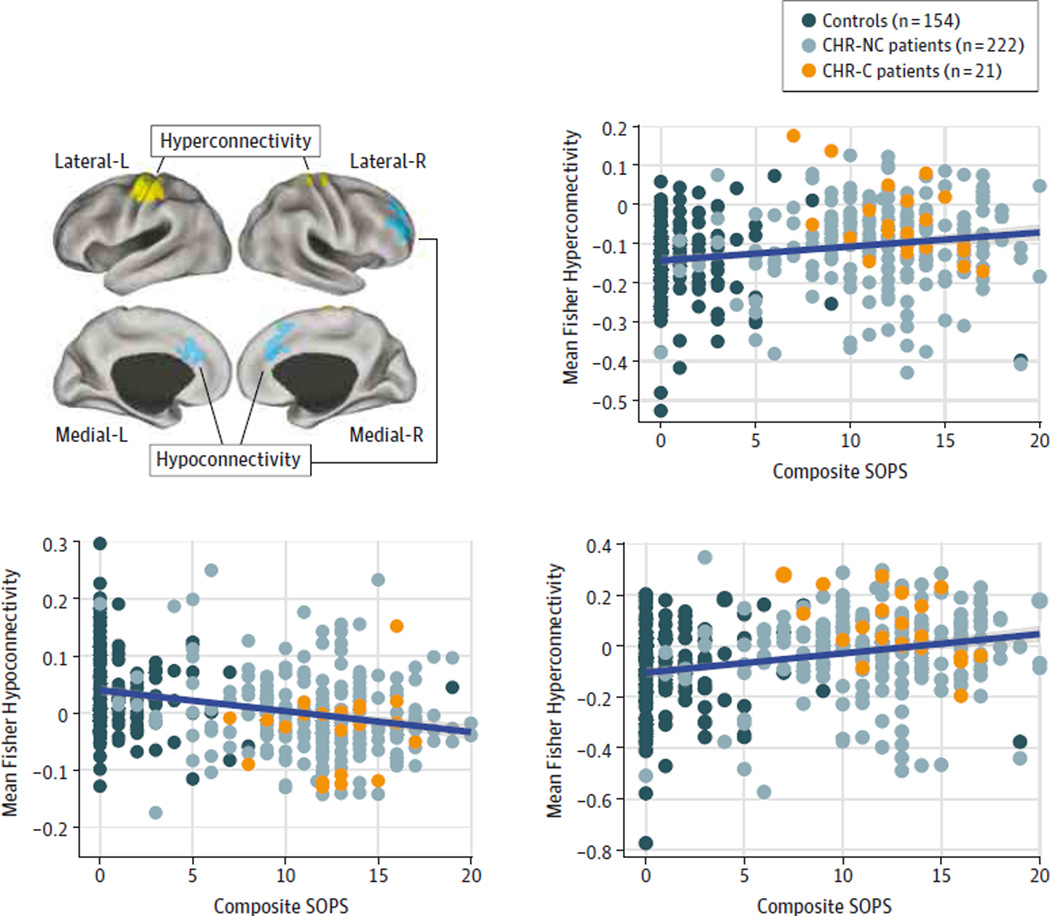
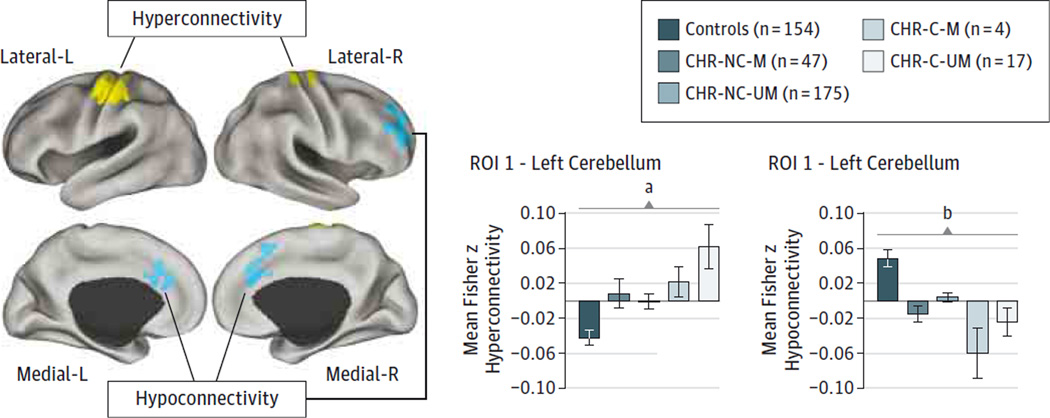
Results: Using baseline magnetic resonance images, we identified thalamocortical dysconnectivity in the 243 individuals at clinical high risk for psychosis, which was particularly pronounced in the 21 participants who converted to full-blown illness. The pattern involved widespread hypoconnectivity between the thalamus and prefrontal and cerebellar areas, which was more prominent in those who converted to full-blown illness (t(173) = 3.77, P < .001, Hedge g = 0.88). Conversely, there was marked thalamic hyperconnectivity with sensory motor areas, again most pronounced in those who converted to full-blown illness (t(173) = 2.85, P < .001, Hedge g = 0.66). Both patterns were significantly correlated with concurrent prodromal symptom severity (r = 0.27, P < 3.6 × 10(-8), Spearman ρ = 0.27, P < 4.75 × 10(-5), 2-tailed).
Conclusions and relevance: Thalamic dysconnectivity, resembling that seen in schizophrenia, was evident in individuals at clinical high risk for psychosis and more prominently in those who later converted to psychosis. Dysconnectivity correlated with symptom severity, supporting the idea that thalamic connectivity may have prognostic implications for risk of conversion to full-blown illness.
Conflict of interest statement
Figures
Comment in
-
The Enduring Search for the Koplik Spots of Psychosis.JAMA Psychiatry. 2015 Sep;72(9):863-4. doi: 10.1001/jamapsychiatry.2015.0611. JAMA Psychiatry. 2015. PMID: 26266967 No abstract available.
References
-
- Weinberger DR. Implications of normal brain development for the pathogenesis of schizophrenia. Arch Gen Psychiatry. 1987;44(7):660–669. - PubMed
-
- Stephan KE, Baldeweg T, Friston KJ. Synaptic plasticity and dysconnection in schizophrenia. Biol Psychiatry. 2006;59(10):929–939. - PubMed
-
- Walker E, Kestler L, Bollini A, Hochman KM. Schizophrenia: etiology and course. Annu Rev Psychol. 2004;55:401–430. - PubMed
-
- Murray CJL, Lopez AD. The Global Burden of Disease: A Comprehensive Assessment of Mortality and Disability From Diseases, Injuries and Risk Factors in 1990 and Projected to 2020. Vol. 1. Cambridge, MA: Harvard University Press; 1996.
Publication types
MeSH terms
Grants and funding
- MH081902/MH/NIMH NIH HHS/United States
- MH081928/MH/NIMH NIH HHS/United States
- DP5 OD012109/OD/NIH HHS/United States
- U01 MH081988/MH/NIMH NIH HHS/United States
- R03 MH105765/MH/NIMH NIH HHS/United States
- F30 MH107149/MH/NIMH NIH HHS/United States
- MH082022/MH/NIMH NIH HHS/United States
- U01 MH066160/MH/NIMH NIH HHS/United States
- K01 MH099431/MH/NIMH NIH HHS/United States
- DP5OD012109-02/OD/NIH HHS/United States
- MH081857/MH/NIMH NIH HHS/United States
- R01 MH108590/MH/NIMH NIH HHS/United States
- U01 MH081928/MH/NIMH NIH HHS/United States
- MH066160/MH/NIMH NIH HHS/United States
- U01 MH082022/MH/NIMH NIH HHS/United States
- U01 MH081984/MH/NIMH NIH HHS/United States
- MH081988/MH/NIMH NIH HHS/United States
- U01 MH081902/MH/NIMH NIH HHS/United States
- T32GM007205/GM/NIGMS NIH HHS/United States
- MH081984/MH/NIMH NIH HHS/United States
- U01 MH076989/MH/NIMH NIH HHS/United States
- T32 GM007205/GM/NIGMS NIH HHS/United States
- MH082004/MH/NIMH NIH HHS/United States
- U01 MH081857/MH/NIMH NIH HHS/United States
- U01 MH082004/MH/NIMH NIH HHS/United States
- U01 MH081944/MH/NIMH NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
