

Troponin and Cardiac Events in Stable Ischemic Heart Disease and Diabetes
- PMID: 26267622
- PMCID: PMC4627639
- DOI: 10.1056/NEJMoa1415921
Troponin and Cardiac Events in Stable Ischemic Heart Disease and Diabetes
Abstract
Background: Cardiac troponin concentrations are used to identify patients who would benefit from urgent revascularization for acute coronary syndromes. We hypothesized that they might be used in patients with stable ischemic heart disease to identify those at high risk for cardiovascular events who might also benefit from prompt coronary revascularization.
Methods: We measured the cardiac troponin T concentration at baseline with a high-sensitivity assay in 2285 patients who had both type 2 diabetes and stable ischemic heart disease and were enrolled in the Bypass Angioplasty Revascularization Investigation in Type 2 Diabetes trial. We tested for an association between the troponin T concentration and a composite end point of death from cardiovascular causes, myocardial infarction, or stroke; we then evaluated whether random assignment to prompt revascularization reduced the rate of the composite end point in patients with an abnormal troponin T concentration (≥14 ng per liter) as compared with those with a normal troponin T concentration (<14 ng per liter).
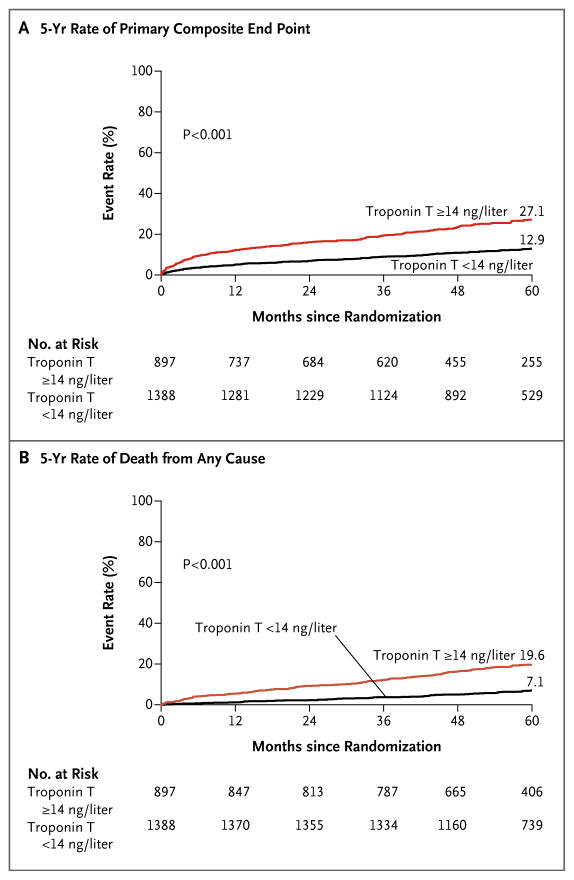
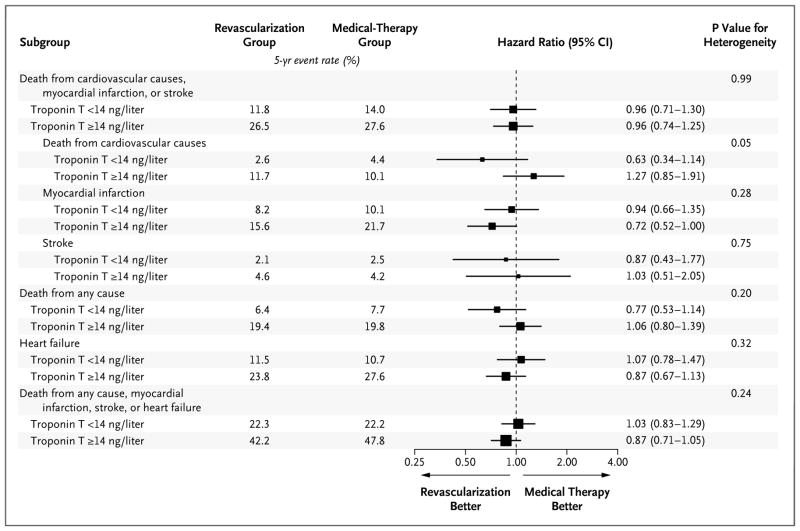
Results: Of the 2285 patients, 2277 (99.6%) had detectable (≥3 ng per liter) troponin T concentrations and 897 (39.3%) had abnormal troponin T concentrations at baseline. The 5-year rate of the composite end point was 27.1% among the patients who had had abnormal troponin T concentrations at baseline, as compared with 12.9% among those who had had normal baseline troponin T concentrations. In models that were adjusted for cardiovascular risk factors, severity of diabetes, electrocardiographic abnormalities, and coronary anatomy, the hazard ratio for the composite end point among patients with abnormal troponin T concentrations was 1.85 (95% confidence interval [CI], 1.48 to 2.32; P<0.001). Among patients with abnormal troponin T concentrations, random assignment to prompt revascularization, as compared with medical therapy alone, did not result in a significant reduction in the rate of the composite end point (hazard ratio, 0.96; 95% CI, 0.74 to 1.25).
Conclusions: The cardiac troponin T concentration was an independent predictor of death from cardiovascular causes, myocardial infarction, or stroke in patients who had both type 2 diabetes and stable ischemic heart disease. An abnormal troponin T value of 14 ng per liter or higher did not identify a subgroup of patients who benefited from random assignment to prompt coronary revascularization. (Funded by the National Institutes of Health and Roche Diagnostics; BARI 2D ClinicalTrials.gov number, NCT00006305.).
Conflict of interest statement
No other potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Cardiac Troponin and Risk Stratification in Ischemic Heart Disease.N Engl J Med. 2015 Aug 13;373(7):672-4. doi: 10.1056/NEJMe1506298. N Engl J Med. 2015. PMID: 26267628 No abstract available.
-
Troponin in Stable Ischemic Heart Disease and Diabetes.N Engl J Med. 2015 Nov 12;373(20):1978-9. doi: 10.1056/NEJMc1511645. N Engl J Med. 2015. PMID: 26559577 No abstract available.
-
Troponin in Stable Ischemic Heart Disease and Diabetes.N Engl J Med. 2015 Nov 12;373(20):1976. doi: 10.1056/NEJMc1511645. N Engl J Med. 2015. PMID: 26559578 No abstract available.
-
Troponin in Stable Ischemic Heart Disease and Diabetes.N Engl J Med. 2015 Nov 12;373(20):1976-7. doi: 10.1056/NEJMc1511645. N Engl J Med. 2015. PMID: 26559579 No abstract available.
-
Troponin in Stable Ischemic Heart Disease and Diabetes.N Engl J Med. 2015 Nov 12;373(20):1977. doi: 10.1056/NEJMc1511645. N Engl J Med. 2015. PMID: 26559580 No abstract available.
-
Troponin in Stable Ischemic Heart Disease and Diabetes.N Engl J Med. 2015 Nov 12;373(20):1977-8. doi: 10.1056/NEJMc1511645. N Engl J Med. 2015. PMID: 26559581 No abstract available.
-
High-sensitivity troponin predicts coronary disease outcomes in type 2 diabetes but yields no benefit in selecting patients for revascularisation.Evid Based Med. 2016 Jun;21(3):100. doi: 10.1136/ebmed-2016-110405. Epub 2016 Apr 13. Evid Based Med. 2016. PMID: 27075268 No abstract available.
References
-
- Thygesen K, Alpert JS, Jaffe AS, et al. Third universal definition of myocardial infarction. J Am Coll Cardiol. 2012;60:1581–98. - PubMed
-
- Morrow DA, Cannon CP, Rifai N, et al. Ability of minor elevations of troponins I and T to predict benefit from an early invasive strategy in patients with unstable angina and non-ST elevation myocardial infarction: results from a randomized trial. JAMA. 2001;286:2405–12. - PubMed
-
- Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC Guideline for the Management of Patients with Non-ST-Elevation Acute Coronary Syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64(24):e139–e228. - PubMed
-
- Bhatt DL, Roe MT, Peterson ED, et al. Utilization of early invasive management strategies for high-risk patients with non-ST-segment elevation acute coronary syndromes: results from the CRUSADE Quality Improvement Initiative. JAMA. 2004;292:2096–104. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical