

A Randomized Trial of Intrapartum Fetal ECG ST-Segment Analysis
- PMID: 26267623
- PMCID: PMC4631435
- DOI: 10.1056/NEJMoa1500600
A Randomized Trial of Intrapartum Fetal ECG ST-Segment Analysis
Abstract
Background: It is unclear whether using fetal electrocardiographic (ECG) ST-segment analysis as an adjunct to conventional intrapartum electronic fetal heart-rate monitoring modifies intrapartum and neonatal outcomes.
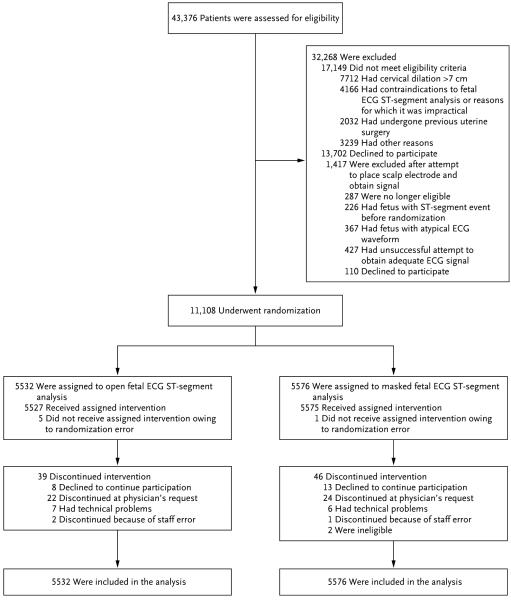
Methods: We performed a multicenter trial in which women with a singleton fetus who were attempting vaginal delivery at more than 36 weeks of gestation and who had cervical dilation of 2 to 7 cm were randomly assigned to "open" or "masked" monitoring with fetal ST-segment analysis. The masked system functioned as a normal fetal heart-rate monitor. The open system displayed additional information for use when uncertain fetal heart-rate patterns were detected. The primary outcome was a composite of intrapartum fetal death, neonatal death, an Apgar score of 3 or less at 5 minutes, neonatal seizure, an umbilical-artery blood pH of 7.05 or less with a base deficit of 12 mmol per liter or more, intubation for ventilation at delivery, or neonatal encephalopathy.
Results: A total of 11,108 patients underwent randomization; 5532 were assigned to the open group, and 5576 to the masked group. The primary outcome occurred in 52 fetuses or neonates of women in the open group (0.9%) and 40 fetuses or neonates of women in the masked group (0.7%) (relative risk, 1.31; 95% confidence interval, 0.87 to 1.98; P=0.20). Among the individual components of the primary outcome, only the frequency of a 5-minute Apgar score of 3 or less differed significantly between neonates of women in the open group and those in the masked group (0.3% vs. 0.1%, P=0.02). There were no significant between-group differences in the rate of cesarean delivery (16.9% and 16.2%, respectively; P=0.30) or any operative delivery (22.8% and 22.0%, respectively; P=0.31). Adverse events were rare and occurred with similar frequency in the two groups.
Conclusions: Fetal ECG ST-segment analysis used as an adjunct to conventional intrapartum electronic fetal heart-rate monitoring did not improve perinatal outcomes or decrease operative-delivery rates. (Funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development and Neoventa Medical; ClinicalTrials.gov number, NCT01131260.).
Figures
Comment in
-
Intrapartum Fetal ECG ST-Segment Analysis.N Engl J Med. 2015 Dec 17;373(25):2480-1. doi: 10.1056/NEJMc1513251. N Engl J Med. 2015. PMID: 26672861 No abstract available.
-
Intrapartum Fetal ECG ST-Segment Analysis.N Engl J Med. 2015 Dec 17;373(25):2480. doi: 10.1056/NEJMc1513251. N Engl J Med. 2015. PMID: 26672862 No abstract available.
-
Adjunctive use of intrapartum foetal ST-segment analysis (STAN) confers no benefit over conventional foetal heart rate monitoring.Evid Based Med. 2016 Jun;21(3):105-6. doi: 10.1136/ebmed-2015-110304. Epub 2016 Mar 16. Evid Based Med. 2016. PMID: 26984285 No abstract available.
References
-
- Food and Drug Administration Approval letter — STAN S31 fetal heart monitor. 2005 Nov 1; http://www.accessdata.fda.gov/cdrh_docs/pdf2/p020001a.pdf.
-
- Rosén KG, Isaksson O. Alterations in fetal heart rate and ECG correlated to glycogen, creatine phosphate and ATP levels during graded hypoxia. Biol Neonate. 1976;30:17–24.
-
- Hökegård KH, Eriksson BO, Kjellmer I, Magno R, Rosén KG. Myocardial metabolism in relation to electrocardiographic changes and cardiac function during graded hypoxia in the fetal lamb. Acta Physiol Scand. 1981;113:1–7. - PubMed
-
- Gelli MG, Bergström J, Hultman E, Thalme B. Heart muscle and plasma electrolytes in normal and glucose-loaded rabbit foetuses under anoxia. Acta Obstet Gynecol Scand. 1969;48:34–55. - PubMed
-
- Watanabe T, Okamura K, Tanigawara S, et al. Change in electrocardiogram T-wave amplitude during umbilical cord compression is predictive of fetal condition in sheep. Am J Obstet Gynecol. 1992;166:246–55. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- HD36801/HD/NICHD NIH HHS/United States
- U10 HD040500/HD/NICHD NIH HHS/United States
- U10 HD040544/HD/NICHD NIH HHS/United States
- HD27869/HD/NICHD NIH HHS/United States
- UG1 HD040560/HD/NICHD NIH HHS/United States
- UG1 HD053097/HD/NICHD NIH HHS/United States
- UG1 HD027915/HD/NICHD NIH HHS/United States
- U10 HD040485/HD/NICHD NIH HHS/United States
- HD68268/HD/NICHD NIH HHS/United States
- HD40545/HD/NICHD NIH HHS/United States
- HD40485/HD/NICHD NIH HHS/United States
- HD40560/HD/NICHD NIH HHS/United States
- U10 HD027917/HD/NICHD NIH HHS/United States
- U10 HD040560/HD/NICHD NIH HHS/United States
- U10 HD040512/HD/NICHD NIH HHS/United States
- U01 HD036801/HD/NICHD NIH HHS/United States
- UG1 HD027869/HD/NICHD NIH HHS/United States
- U10 HD068268/HD/NICHD NIH HHS/United States
- HD68282/HD/NICHD NIH HHS/United States
- HD40512/HD/NICHD NIH HHS/United States
- UG1 HD040544/HD/NICHD NIH HHS/United States
- UG1 HD034208/HD/NICHD NIH HHS/United States
- UG1 HD040512/HD/NICHD NIH HHS/United States
- HD21410/HD/NICHD NIH HHS/United States
- U10 HD027869/HD/NICHD NIH HHS/United States
- U10 HD027915/HD/NICHD NIH HHS/United States
- U10 HD068282/HD/NICHD NIH HHS/United States
- UG1 HD040545/HD/NICHD NIH HHS/United States
- UG1 HD040485/HD/NICHD NIH HHS/United States
- UG1 HD068268/HD/NICHD NIH HHS/United States
- HD40500/HD/NICHD NIH HHS/United States
- U10 HD034208/HD/NICHD NIH HHS/United States
- U10 HD053097/HD/NICHD NIH HHS/United States
- HD34208/HD/NICHD NIH HHS/United States
- HD27915/HD/NICHD NIH HHS/United States
- UG1 HD040500/HD/NICHD NIH HHS/United States
- UG1 HD068282/HD/NICHD NIH HHS/United States
- HD27917/HD/NICHD NIH HHS/United States
- U10 HD021410/HD/NICHD NIH HHS/United States
- U24 HD036801/HD/NICHD NIH HHS/United States
- U10 HD036801/HD/NICHD NIH HHS/United States
- HD53097/HD/NICHD NIH HHS/United States
- U10 HD040545/HD/NICHD NIH HHS/United States
- HD40544/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical