

Iatrogenic CJD due to pituitary-derived growth hormone with genetically determined incubation times of up to 40 years
- PMID: 26268531
- PMCID: PMC4620512
- DOI: 10.1093/brain/awv235
Iatrogenic CJD due to pituitary-derived growth hormone with genetically determined incubation times of up to 40 years
Abstract
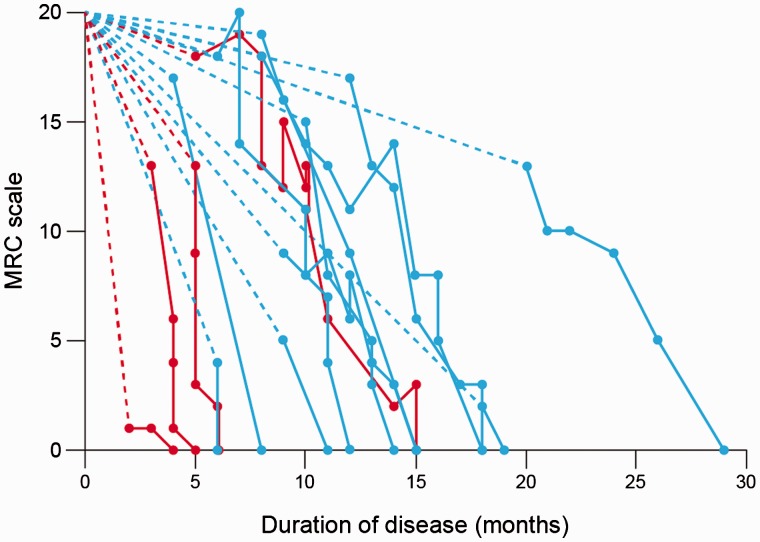
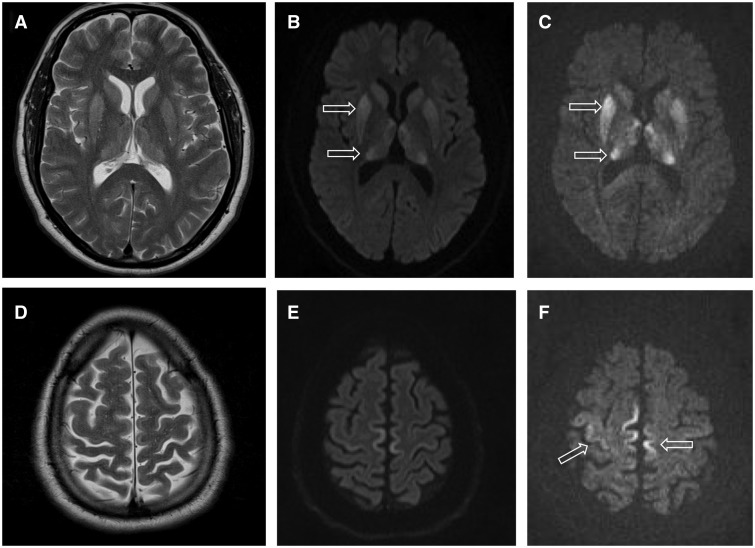
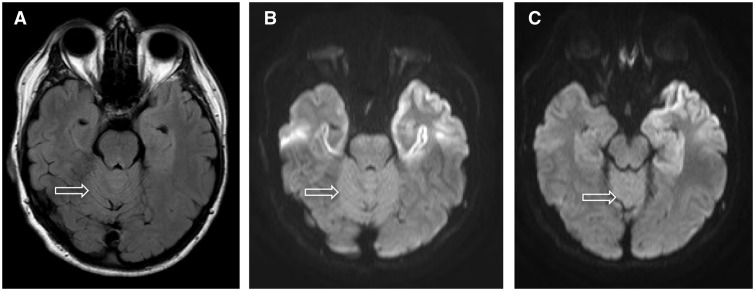
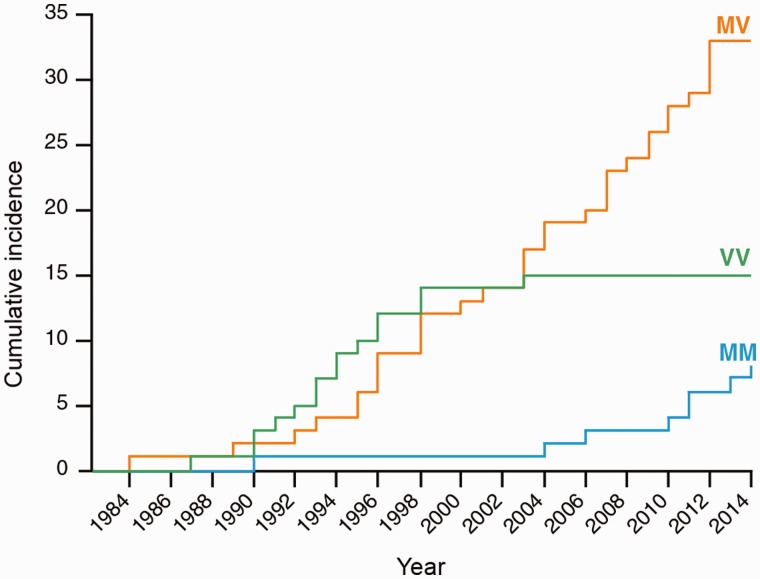
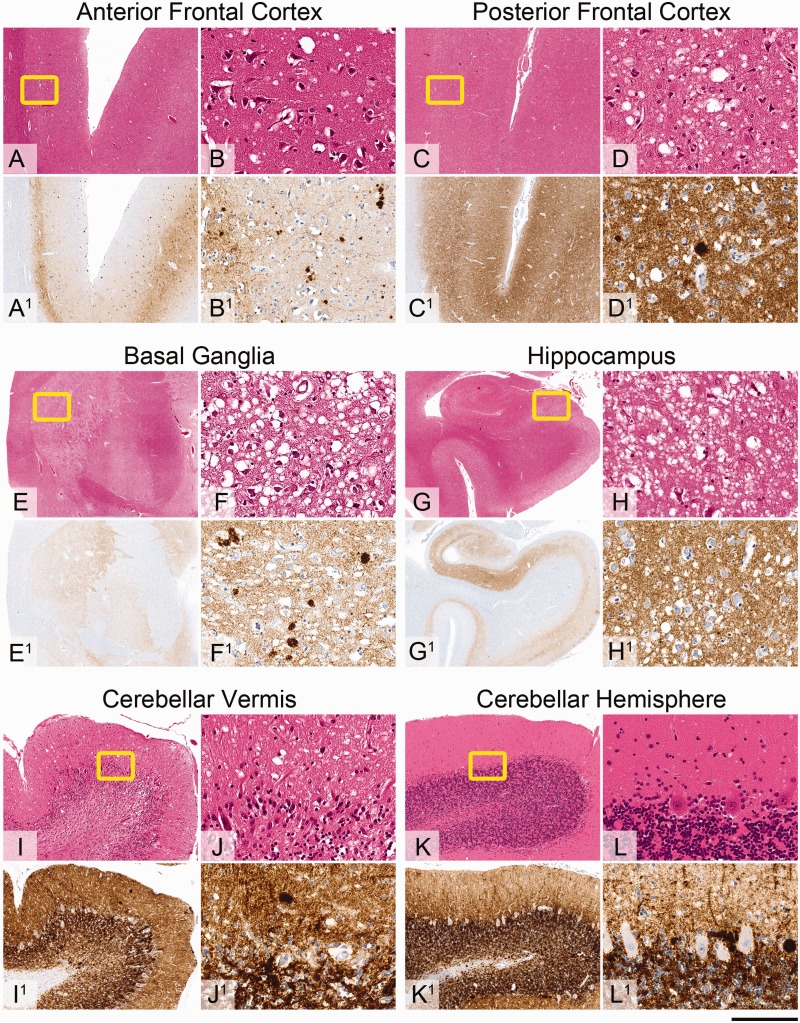
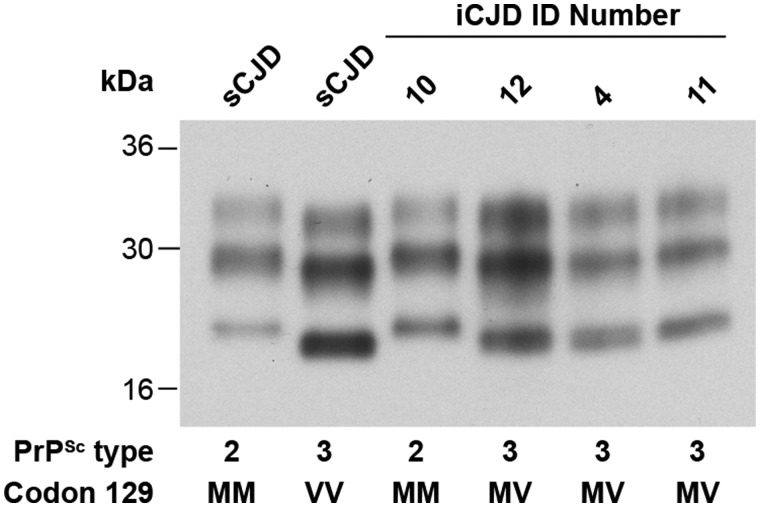
Patients with iatrogenic Creutzfeldt-Jakob disease due to administration of cadaver-sourced growth hormone during childhood are still being seen in the UK 30 years after cessation of this treatment. Of the 77 patients who have developed iatrogenic Creutzfeldt-Jakob disease, 56 have been genotyped. There has been a marked change in genotype profile at polymorphic codon 129 of the prion protein gene (PRNP) from predominantly valine homozygous to a mixed picture of methionine homozygous and methionine-valine heterozygous over time. The incubation period of iatrogenic Creutzfeldt-Jakob disease is significantly different between all three genotypes. This experience is a striking contrast with that in France and the USA, which may relate to contamination of different growth hormone batches with different strains of human prions. We describe the clinical, imaging, molecular and autopsy features in 22 of 24 patients who have developed iatrogenic Creutzfeldt-Jakob disease in the UK since 2003. Mean age at onset of symptoms was 42.7 years. Gait ataxia and lower limb dysaesthesiae were the most frequent presenting symptoms. All had cerebellar signs, and the majority had myoclonus and lower limb pyramidal signs, with relatively preserved cognitive function, when first seen. There was a progressive decline in neurological and cognitive function leading to death after 5-32 (mean 14) months. Despite incubation periods approaching 40 years, the clinical duration in methionine homozygote patients appeared to be shorter than that seen in heterozygote patients. MRI showed restricted diffusion in the basal ganglia, thalamus, hippocampus, frontal and the paracentral motor cortex and cerebellar vermis. The electroencephalogram was abnormal in 15 patients and cerebrospinal fluid 14-3-3 protein was positive in half the patients. Neuropathological examination was conducted in nine patients. All but one showed synaptic prion deposition with numerous kuru type plaques in the basal ganglia, anterior frontal and parietal cortex, thalamus, basal ganglia and cerebellum. The patient with the shortest clinical duration had an atypical synaptic deposition of abnormal prion protein and no kuru plaques. Taken together, these data provide a remarkable example of the interplay between the strain of the pathogen and host prion protein genotype. Based on extensive modelling of human prion transmission barriers in transgenic mice expressing human prion protein on a mouse prion protein null background, the temporal distribution of codon 129 genotypes within the cohort of patients with iatrogenic Creutzfeldt-Jakob disease in the UK suggests that there was a point source of infecting prion contamination of growth hormone derived from a patient with Creutzfeldt-Jakob disease expressing prion protein valine 129.
Keywords: PRNP; RRP9; growth hormone; iatrogenic Creutzfeldt-Jakob disease; prion disease.
© The Author (2015). Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures
References
-
- Brandel JP, Preece M, Brown P, Croes E, Laplanche JL, Agid Y, et al. Distribution of codon 129 genotype in human growth hormone-treated CJD patients in France and the UK. Lancet 2003; 362: 128–30. - PubMed
-
- Brandner S. Diversity of prion diseases: (no) strains attached? Acta Neuropathol 2011; 121: 1–4. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
