

Pain typology and incident endometriosis
- PMID: 26269529
- PMCID: PMC4573450
- DOI: 10.1093/humrep/dev147
Pain typology and incident endometriosis
Abstract
Study question: What are the pain characteristics among women, with no prior endometriosis diagnosis, undergoing laparoscopy or laparotomy regardless of clinical indication?
Summary answer: Women with surgically visualized endometriosis reported the highest chronic/cyclic pain and significantly greater dyspareunia, dysmenorrhea, and dyschezia compared with women with other gynecologic pathology (including uterine fibroids, pelvic adhesions, benign ovarian cysts, neoplasms and congenital Müllerian anomalies) or a normal pelvis.
What is known already: Prior research has shown that various treatments for pain associated with endometriosis can be effective, making identification of specific pain characteristics in relation to endometriosis necessary for informing disease diagnosis and management.
Study design, size, duration: The study population for these analyses includes the ENDO Study (2007-2009) operative cohort: 473 women, ages 18-44 years, who underwent a diagnostic and/or therapeutic laparoscopy or laparotomy at one of 14 surgical centers located in Salt Lake City, UT or San Francisco, CA. Women with a history of surgically confirmed endometriosis were excluded.
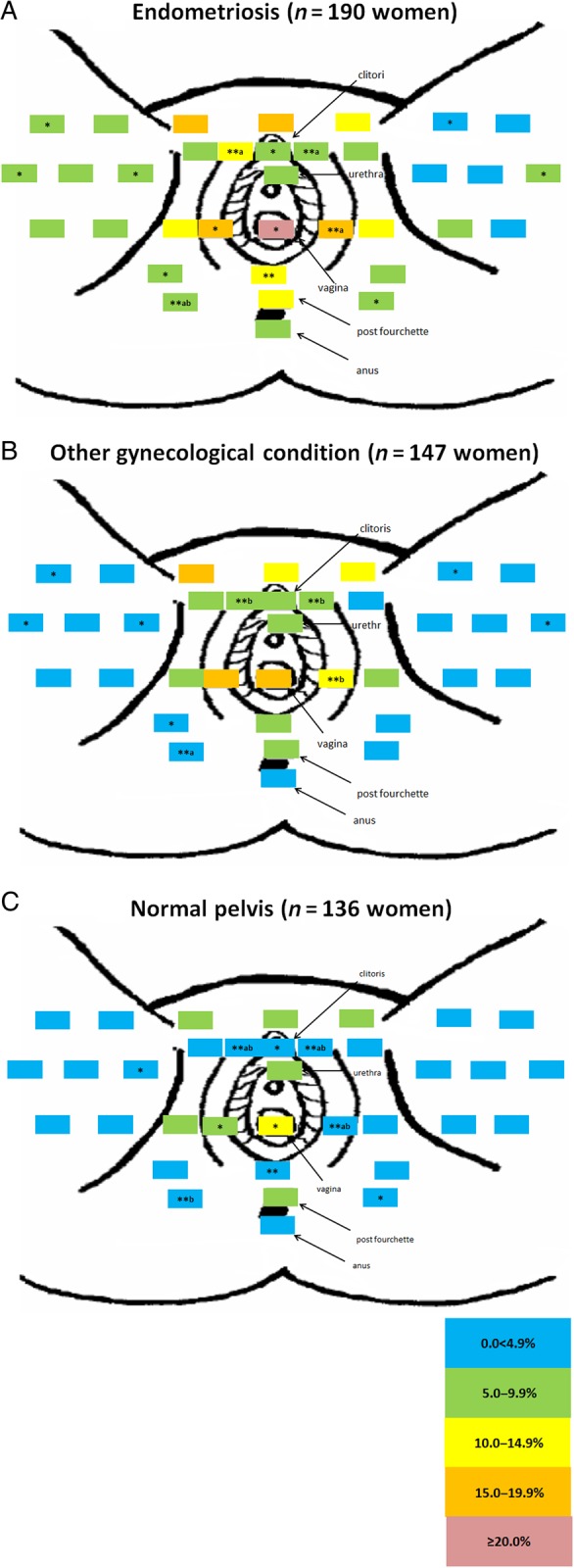
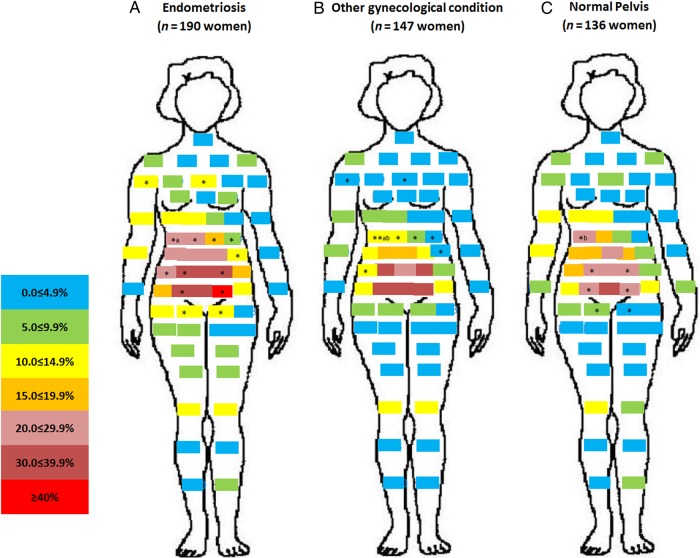
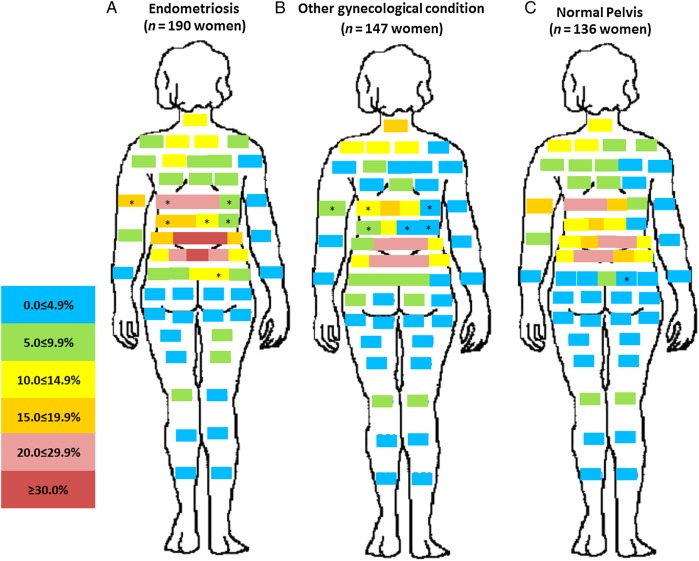
Participants/materials, setting and methods: Endometriosis was defined as surgically visualized disease; staging was based on revised American Society for Reproductive Medicine (rASRM) criteria. All women completed a computer-assisted personal interview at baseline specifying 17 types of pain (rating severity via 11-point visual analog scale) and identifying any of 35 perineal and 60 full-body front and 60 full-body back sites for which they experienced pain in the last 6 months.
Main results and the role of chance: There was a high prevalence (≥30%) of chronic and cyclic pelvic pain reported by the entire study cohort regardless of post-operative diagnosis. However, women with a post-operative endometriosis diagnosis, compared with women diagnosed with other gynecologic disorders or a normal pelvis, reported more cyclic pelvic pain (49.5% versus 31.0% and 33.1%, P < 0.001). Additionally, women with endometriosis compared with women with a normal pelvis experienced more chronic pain (44.2 versus 30.2%, P = 0.04). Deep pain with intercourse, cramping with periods, and pain with bowel elimination were much more likely reported in women with versus without endometriosis (all P < 0.002). A higher percentage of women diagnosed with endometriosis compared with women with a normal pelvis reported vaginal (22.6 versus 10.3%, P < 0.01), right labial (18.4 versus 8.1%, P < 0.05) and left labial pain (15.3 versus 3.7%, P < 0.01) along with pain in the right/left hypogastric and umbilical abdominopelvic regions (P < 0.05 for all). Among women with endometriosis, no clear and consistent patterns emerged regarding pain characteristics and endometriosis staging or anatomic location.
Limitations, reasons for caution: Interpretation of our findings requires caution given that we were limited in our assessment of pain characteristics by endometriosis staging and anatomic location due to the majority of women having minimal (stage I) disease (56%) and lesions in peritoneum-only location (51%). Significance tests for pain topology related to gynecologic pathology were not corrected for multiple comparisons.
Wider implications of the findings: Results of our research suggest that while women with endometriosis appear to have higher pelvic pain, particularly dyspareunia, dysmenorrhea, dyschezia and pain in the vaginal and abdominopelvic area than women with other gynecologic disorders or a normal pelvis, pelvic pain is commonly reported among women undergoing laparoscopy, even among women with no identified gynecologic pathology. Future research should explore causes of pelvic pain among women who seek out gynecologic care but with no apparent gynecologic pathology. Given our and other's research showing little correlation between pelvic pain and rASRM staging among women with endometriosis, further development and use of a classification system that can better predict outcomes for endometriosis patients with pelvic pain for both surgical and nonsurgical treatment is needed.
Study funding/competing interests: Supported by the Intramural Research Program, Eunice Kennedy Shriver National Institute of Child Health and Human Development (contracts NO1-DK-6-3428, NO1-DK-6-3427, and 10001406-02). The authors have no potential competing interests.
Keywords: dysmenorrhea; dyspareunia; endometriosis; epidemiology; laparoscopy.
© The Author 2015. Published by Oxford University Press on behalf of the European Society of Human Reproduction and Embryology. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Adamson GD. Endometriosis classification: an update. Curr Opin Obstet Gynecol 2011;23:213–220. - PubMed
-
- Adamson GD, Pasta DJ. Endometriosis fertility index: the new, validated endometriosis staging system. Fertil Steril 2010;94:1609–1615. - PubMed
-
- Al-Badawi IA, Fluker MR, Bebbington MW. Diagnostic laparoscopy in infertile women with normal hysterosalpingograms. J Reprod Med 1999;44:953–957. - PubMed
-
- American Society for Reproductive Medicine. Revised American Society for Reproductive Medicine (rASRM) classification of endometriosis: 1996. Fertil Steril 1997;67:817–821. - PubMed
-
- American Society for Reproductive Medicine. Treatment of pelvic pain associated with endometriosis: a committee opinion. Fertil Steril 2014;101:927–935. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
