

Molecular Basis of Hypokalemia-Induced Ventricular Fibrillation
- PMID: 26269574
- PMCID: PMC4618042
- DOI: 10.1161/CIRCULATIONAHA.115.016217
Molecular Basis of Hypokalemia-Induced Ventricular Fibrillation
Abstract
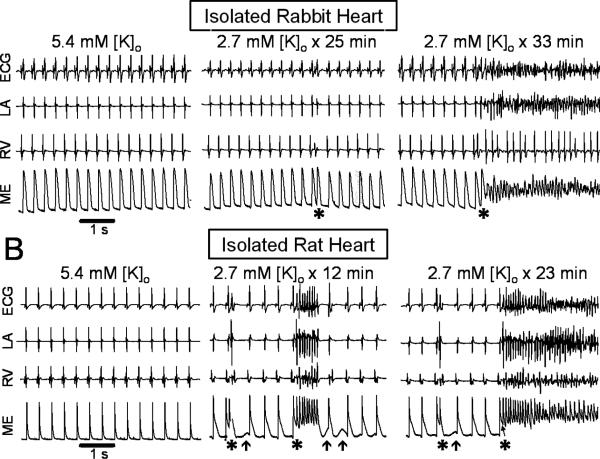
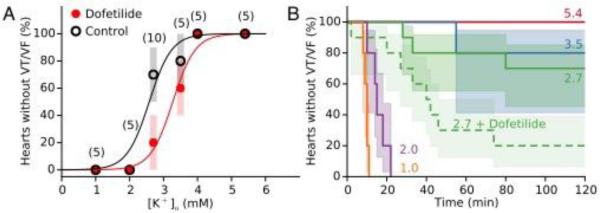
Background: Hypokalemia is known to promote ventricular arrhythmias, especially in combination with class III antiarrhythmic drugs like dofetilide. Here, we evaluated the underlying molecular mechanisms.
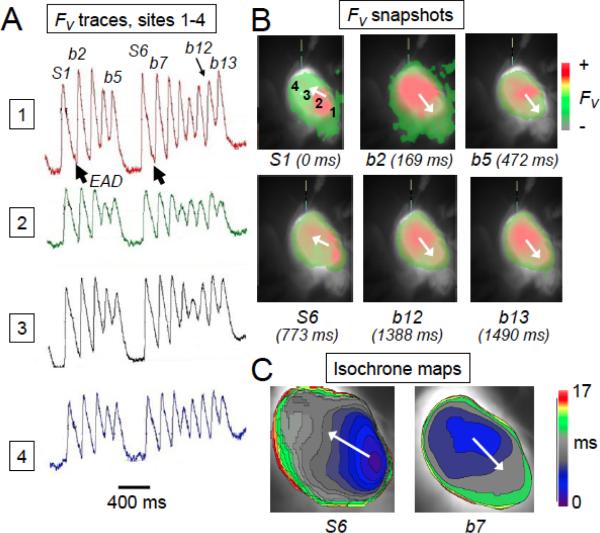
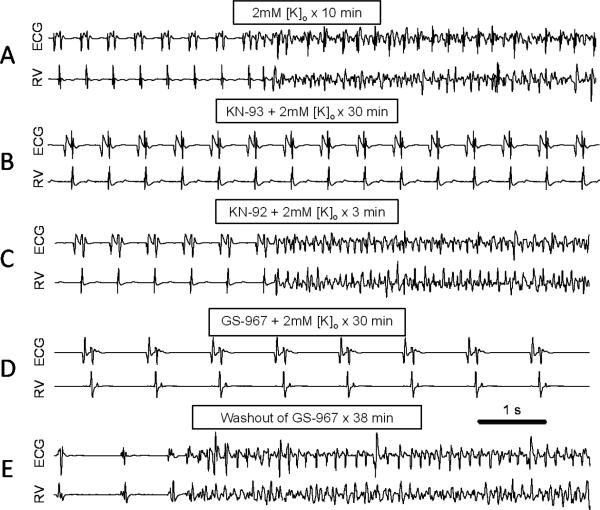
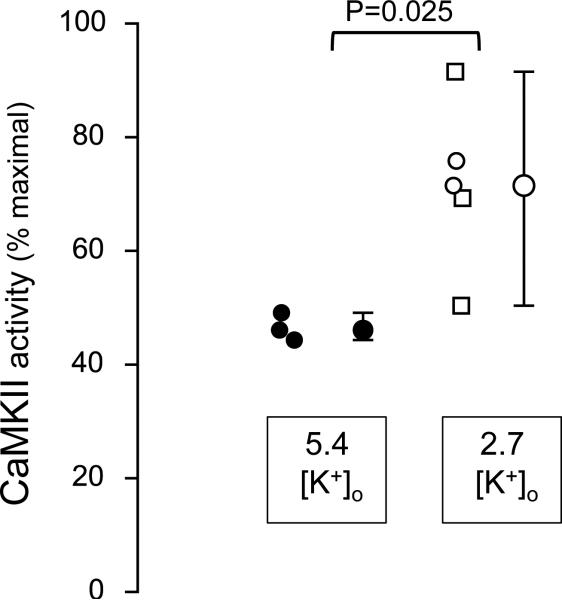
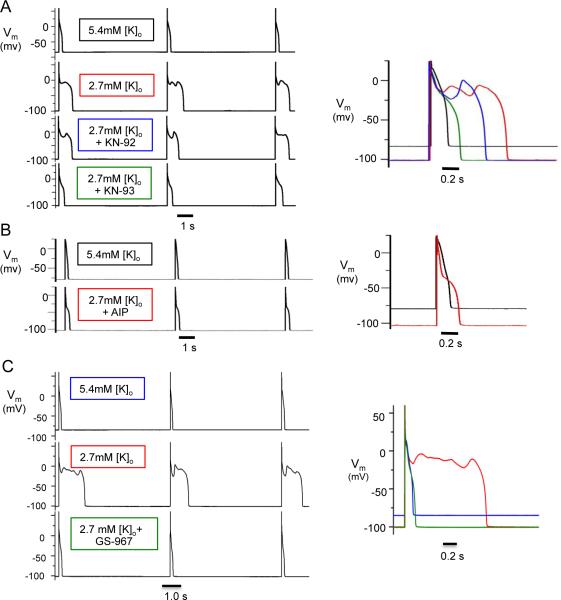
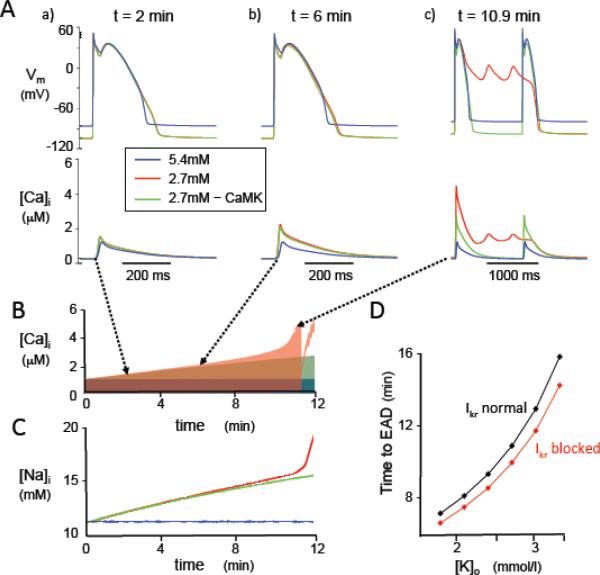
Methods and results: Arrhythmias were recorded in isolated rabbit and rat hearts or patch-clamped ventricular myocytes exposed to hypokalemia (1.0-3.5 mmol/L) in the absence or presence of dofetilide (1 μmol/L). Spontaneous early afterdepolarizations (EADs) and ventricular tachycardia/fibrillation occurred in 50% of hearts at 2.7 mmol/L [K] in the absence of dofetilide and 3.3 mmol/L [K] in its presence. Pretreatment with the Ca-calmodulin kinase II (CaMKII) inhibitor KN-93, but not its inactive analogue KN-92, abolished EADs and hypokalemia-induced ventricular tachycardia/fibrillation, as did the selective late Na current (INa) blocker GS-967. In intact hearts, moderate hypokalemia (2.7 mmol/L) significantly increased tissue CaMKII activity. Computer modeling revealed that EAD generation by hypokalemia (with or without dofetilide) required Na-K pump inhibition to induce intracellular Na and Ca overload with consequent CaMKII activation enhancing late INa and the L-type Ca current. K current suppression by hypokalemia and dofetilide alone in the absence of CaMKII activation were ineffective at causing EADs.
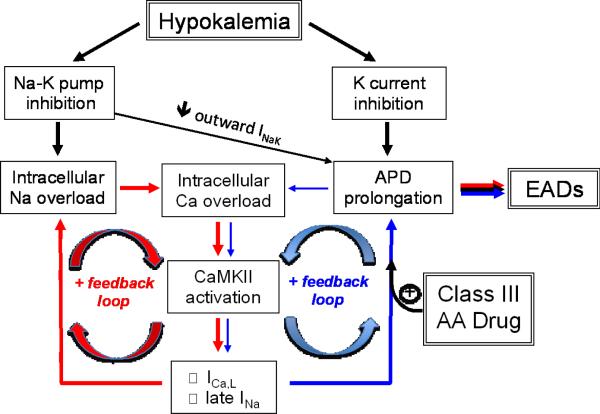
Conclusions: We conclude that Na-K pump inhibition by even moderate hypokalemia plays a critical role in promoting EAD-mediated arrhythmias by inducing a positive feedback cycle activating CaMKII and enhancing late INa. Class III antiarrhythmic drugs like dofetilide sensitize the heart to this positive feedback loop.
Keywords: anti-arrhythmia agents; arrhythmias, cardiac; long QT syndrome; potassium; signal transduction.
© 2015 American Heart Association, Inc.
Figures
References
-
- Schulman M, Narins RG. Hypokalemia and cardiovascular disease. Am J Cardiol. 1990;65:4E–9E. discussion 22E-23E. - PubMed
-
- Macdonald JE, Struthers AD. What is the optimal serum potassium level in cardiovascular patients? J Am Coll Cardiol. 2004;43:155–61. - PubMed
-
- Cooper HA, Dries DL, Davis CE, Shen YL, Domanski MJ. Diuretics and risk of arrhythmic death in patients with left ventricular dysfunction. Circulation. 1999;100:1311–5. - PubMed
-
- Siscovick DS, Raghunathan TE, Psaty BM, Koepsell TD, Wicklund KG, Lin X, Cobb L, Rautaharju PM, Copass MK, Wagner EH. Diuretic therapy for hypertension and the risk of primary cardiac arrest. N Engl J Med. 1994;330:1852–7. - PubMed
-
- Sanguinetti MC, Jurkiewicz NK. Role of external Ca and K in gating of cardiac delayed rectifier K currents. Pflugers Arch. 1992;420:180–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
