

Inflammatory pouch disease: The spectrum of pouchitis
- PMID: 26269664
- PMCID: PMC4528017
- DOI: 10.3748/wjg.v21.i29.8739
Inflammatory pouch disease: The spectrum of pouchitis
Abstract
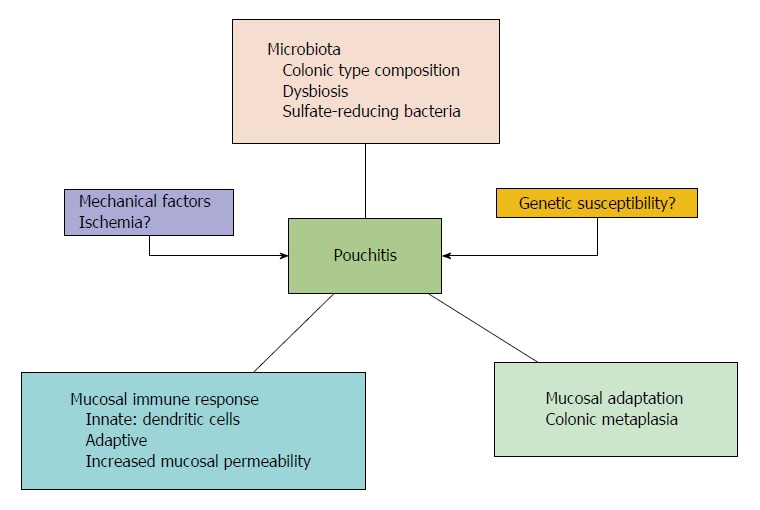
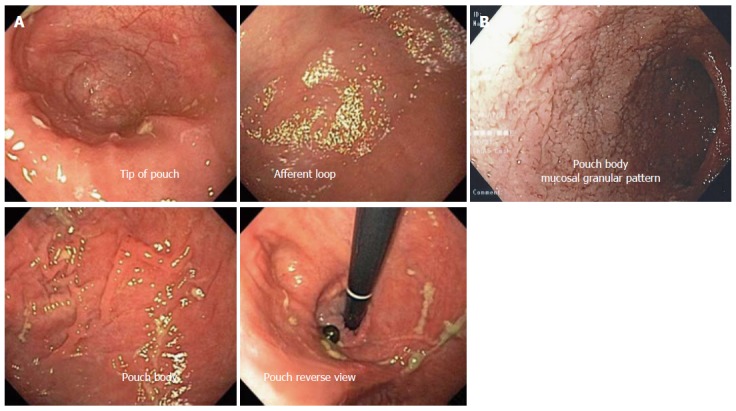
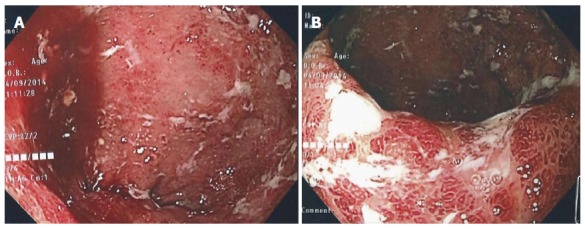
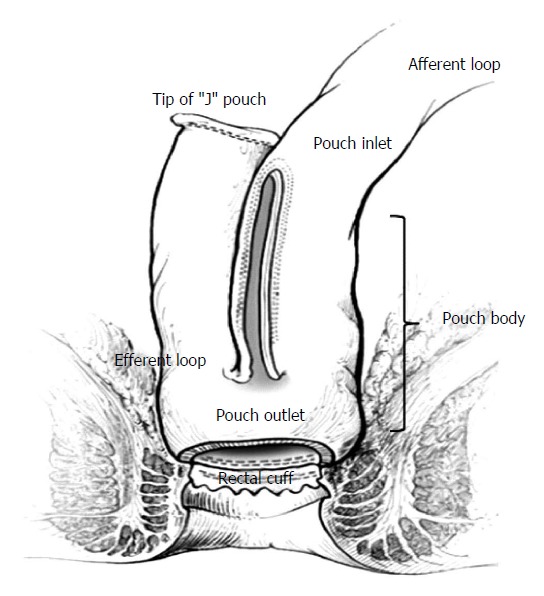
Restorative proctocolectomy with ileal-pouch anal anastomosis (IPAA) is the operation of choice for medically refractory ulcerative colitis (UC), for UC with dysplasia, and for familial adenomatous polyposis (FAP). IPAA can be a treatment option for selected patients with Crohn's colitis without perianal and/or small bowel disease. The term "pouchitis" refers to nonspecific inflammation of the pouch and is a common complication in patients with IPAA; it occurs more often in UC patients than in FAP patients. This suggests that the pathogenetic background of UC may contribute significantly to the development of pouchitis. The symptoms of pouchitis are many, and can include increased bowel frequency, urgency, tenesmus, incontinence, nocturnal seepage, rectal bleeding, abdominal cramps, and pelvic discomfort. The diagnosis of pouchitis is based on the presence of symptoms together with endoscopic and histological evidence of inflammation of the pouch. However, "pouchitis" is a general term representing a wide spectrum of diseases and conditions, which can emerge in the pouch. Based on the etiology we can sub-divide pouchitis into 2 groups: idiopathic and secondary. In idiopathic pouchitis the etiology and pathogenesis are still unclear, while in secondary pouchitis there is an association with a specific causative or pathogenetic factor. Secondary pouchitis can occur in up to 30% of cases and can be classified as infectious, ischemic, non-steroidal anti-inflammatory drugs-induced, collagenous, autoimmune-associated, or Crohn's disease. Sometimes, cuffitis or irritable pouch syndrome can be misdiagnosed as pouchitis. Furthermore, idiopathic pouchitis itself can be sub-classified into types based on the clinical pattern, presentation, and responsiveness to antibiotic treatment. Treatment differs among the various forms of pouchitis. Therefore, it is important to establish the correct diagnosis in order to select the appropriate treatment and further management. In this editorial, we present the spectrum of pouchitis and the specific features related to the diagnosis and treatment of the various forms.
Keywords: Idiopathic pouchitis; Pouchitis; Secondary pouchitis; Ulcerative colitis, Crohn’s disease.
Figures
References
-
- Melton GB, Fazio VW, Kiran RP, He J, Lavery IC, Shen B, Achkar JP, Church JM, Remzi FH. Long-term outcomes with ileal pouch-anal anastomosis and Crohn’s disease: pouch retention and implications of delayed diagnosis. Ann Surg. 2008;248:608–616. - PubMed
-
- Ferrante M, Declerck S, De Hertogh G, Van Assche G, Geboes K, Rutgeerts P, Penninckx F, Vermeire S, D’Hoore A. Outcome after proctocolectomy with ileal pouch-anal anastomosis for ulcerative colitis. Inflamm Bowel Dis. 2008;14:20–28. - PubMed
-
- Shen B, Fazio VW, Remzi FH, Delaney CP, Bennett AE, Achkar JP, Brzezinski A, Khandwala F, Liu W, Bambrick ML, et al. Comprehensive evaluation of inflammatory and noninflammatory sequelae of ileal pouch-anal anastomoses. Am J Gastroenterol. 2005;100:93–101. - PubMed
-
- Seril DN, Yao Q, Shen B. The association between autoimmunity and pouchitis. Inflamm Bowel Dis. 2014;20:378–388. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
