

Comprehensive Cardiovascular Risk Factor Control Improves Survival: The BARI 2D Trial
- PMID: 26271057
- PMCID: PMC4550809
- DOI: 10.1016/j.jacc.2015.06.019
Comprehensive Cardiovascular Risk Factor Control Improves Survival: The BARI 2D Trial
Abstract
Background: It is unclear whether achieving multiple risk factor (RF) goals through protocol-guided intensive medical therapy is feasible or improves outcomes in type 2 diabetes mellitus.
Objectives: This study sought to quantify the relationship between achieved RF goals in the BARI 2D (Bypass Angioplasty Investigation Revascularization 2 Diabetes) trial and cardiovascular events/survival.
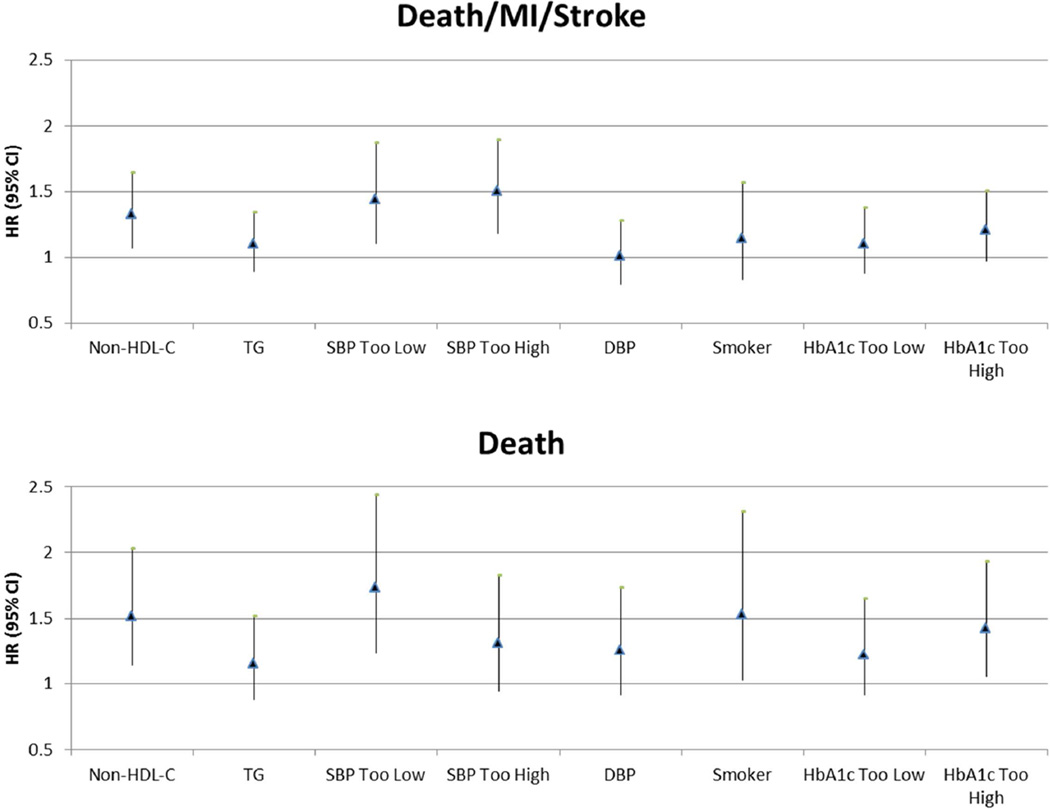
Methods: We performed a nonrandomized analysis of survival/cardiovascular events and control of 6 RFs (no smoking, non-high-density lipoprotein cholesterol <130 mg/dl, triglycerides <150 mg/dl, blood pressure [systolic <130 mm Hg; diastolic <80 mm Hg], glycosylated hemoglobin <7%) in BARI 2D. Cox models with time-varying number of RFs in control were adjusted for baseline number of RFs in control, clinical characteristics, and trial randomization assignments.
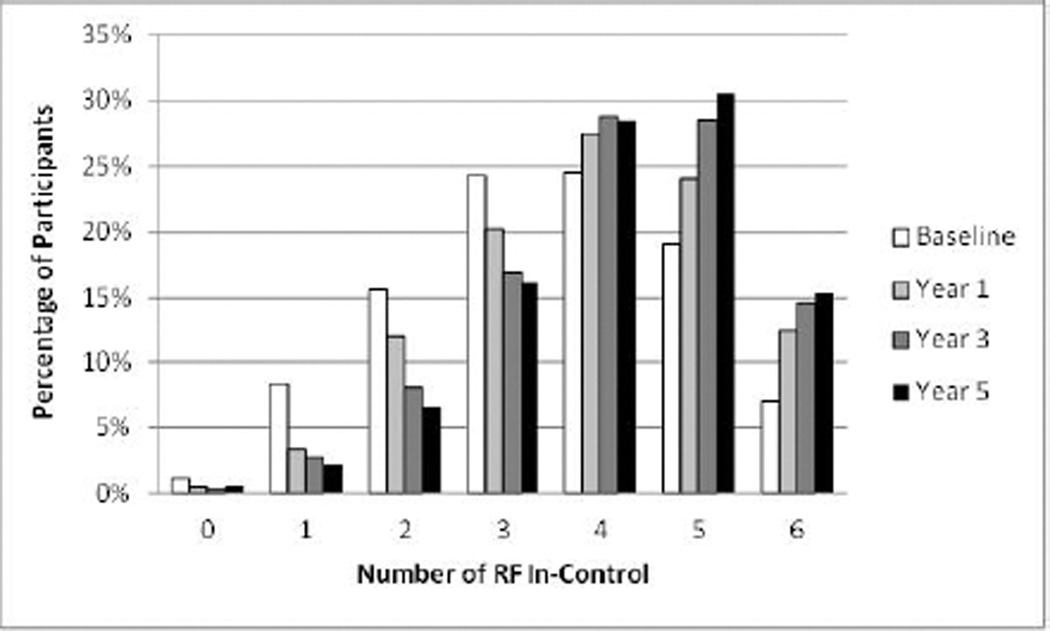
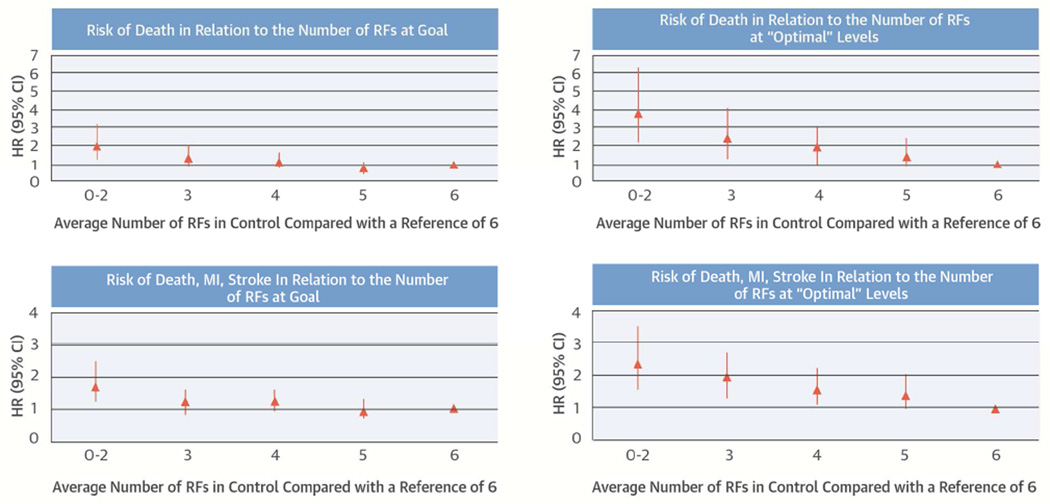
Results: In 2,265 patients (mean age 62 years, 29% women) followed up for 5 years, the mean ± SD number of RFs in control improved from 3.5 ± 1.4 at baseline to 4.2 ± 1.3 at 5 years (p < 0.0001). The number of RFs in control during the trial was strongly related to death (global p = 0.0010) and the composite of death, myocardial infarction, and stroke (global p = 0.0035) in fully adjusted models. Participants with 0 to 2 RFs in control during follow-up had a 2-fold higher risk of death (hazard ratio: 2.0; 95% confidence interval: 1.3 to 3.3; p = 0.0031) and a 1.7-fold higher risk of the composite endpoint (hazard ratio: 1.7; 95% confidence interval: 1.2 to 2.5; p = 0.0043), compared with those with 6 RFs in control.
Conclusions: Simultaneous control of multiple RFs through protocol-guided intensive medical therapy is feasible and relates to cardiovascular morbidity and mortality in patients with coronary disease and type 2 diabetes mellitus. (Bypass Angioplasty Revascularization Investigation in Type 2 Diabetes [BARI 2D]; NCT00006305).
Keywords: blood pressure; cholesterol; coronary heart disease; diabetes mellitus; glycosylated hemoglobin A; smoking.
Copyright © 2015 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Why Optimal Medical Therapy Should Be a Universal Standard of Care.J Am Coll Cardiol. 2015 Aug 18;66(7):774-776. doi: 10.1016/j.jacc.2015.06.018. J Am Coll Cardiol. 2015. PMID: 26271058 Free PMC article. No abstract available.
References
-
- Ford ES, Ajani UA, Croft JB, et al. Explaining the decrease in U.S. deaths from coronary disease, 1980–2000. N Engl J Med. 2007;356:2388–2398. - PubMed
-
- Gaede P, Vedel P, Larsen N, et al. Multifactorial intervention and cardiovascular disease in patients with type 2 diabetes. N Engl J Med. 2003;348:383–393. - PubMed
-
- Gaede P, Lund-Andersen H, Parving HH, et al. Effect of a multifactorial intervention on mortality in type 2 diabetes. N Engl J Med. 2008;358:580–591. - PubMed
Publication types
MeSH terms
Supplementary concepts
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
