

Learning before leaping: integration of an adaptive study design process prior to initiation of BetterBirth, a large-scale randomized controlled trial in Uttar Pradesh, India
- PMID: 26271331
- PMCID: PMC4536663
- DOI: 10.1186/s13012-015-0309-y
Learning before leaping: integration of an adaptive study design process prior to initiation of BetterBirth, a large-scale randomized controlled trial in Uttar Pradesh, India
Abstract
Background: Pragmatic and adaptive trial designs are increasingly used in quality improvement (QI) interventions to provide the strongest evidence for effective implementation and impact prior to broader scale-up. We previously showed that an on-site coaching intervention focused on the World Health Organization Safe Childbirth Checklist (SCC) improved performance of essential birth practices (EBPs) in one facility in Karnataka, India. We report on the process and outcomes of adapting the intervention prior to larger-scale implementation in a randomized controlled trial in Uttar Pradesh (UP), India.
Methods: Initially, we trained a local team of physicians and nurses to coach birth attendants in SCC use at two public facilities for 4-6 weeks. Trained observers evaluated adherence to EBPs before and after coaching. Using mixed methods and a systematic adaptation process, we modified and strengthened the intervention. The modified intervention was implemented in three additional facilities. Pre/post-change in EBP prevalence aggregated across facilities was analyzed.
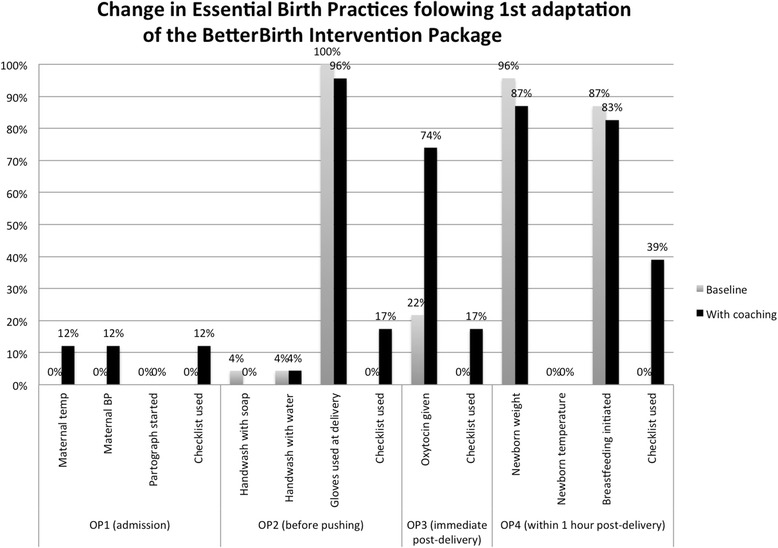
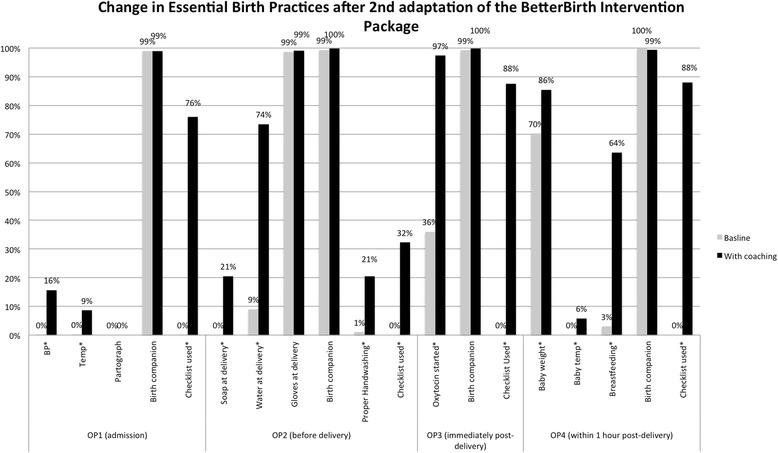
Results: In the first two facilities, limited improvement was seen in EBPs with the exception of post-partum oxytocin. Checklists were used <25 % of observations. We identified challenges in physicians coaching nurses, need to engage district and facility leadership to address system gaps, and inadequate strategy for motivating SCC uptake. Revisions included change to peer-to-peer coaching (nurse to nurse, physician to physician); strengthened coach training on behavior and system change; adapted strategy for effective leadership engagement; and an explicit motivation strategy to enhance professional pride and effectiveness. These modifications resulted in improvement in multiple EBPs from baseline including taking maternal blood pressure (0 to 16 %), post-partum oxytocin (36 to 97 %), early breastfeeding initiation (3 to 64 %), as well as checklist use (range 32 to 88 %), all p < 0.01. Further adaptations were implemented to increase the effectiveness prior to full trial launch.
Conclusions: The adaptive study design of implementation, evaluation, and feedback drove iterative redesign and successfully developed a SCC-focused coaching intervention that improved EBPs in UP facilities. This work was critical to develop a replicable BetterBirth package tailored to the local context. The multi-center pragmatic trial is underway measuring impact of the BetterBirth program on EBP and maternal-neonatal morbidity and mortality.
Clinical trials identifier: NCT02148952 .
Figures
References
-
- Kilbourne AM, Abraham KM, Goodrich DE, Bowersox NW, Almirall D, Lai Z, et al. Cluster randomized adaptive implementation trial comparing a standard versus enhanced implementation intervention to improve uptake of an effective re-engagement program for patients with serious mental illness. Implement Sci. 2013;8:136. doi: 10.1186/1748-5908-8-136. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
