

Incidence of abnormal positron emission tomography in patients with unexplained cardiomyopathy and ventricular arrhythmias: The potential role of occult inflammation in arrhythmogenesis
- PMID: 26272522
- PMCID: PMC4656080
- DOI: 10.1016/j.hrthm.2015.08.014
Incidence of abnormal positron emission tomography in patients with unexplained cardiomyopathy and ventricular arrhythmias: The potential role of occult inflammation in arrhythmogenesis
Abstract
Background: The incidence of myocardial inflammation in patients with unexplained cardiomyopathy referred for ventricular arrhythmias (VAs) is unknown.
Objective: The purpose of this study was to report fasting positron emission tomographic (PET) scan findings in consecutive patients referred with unexplained cardiomyopathy and VA.
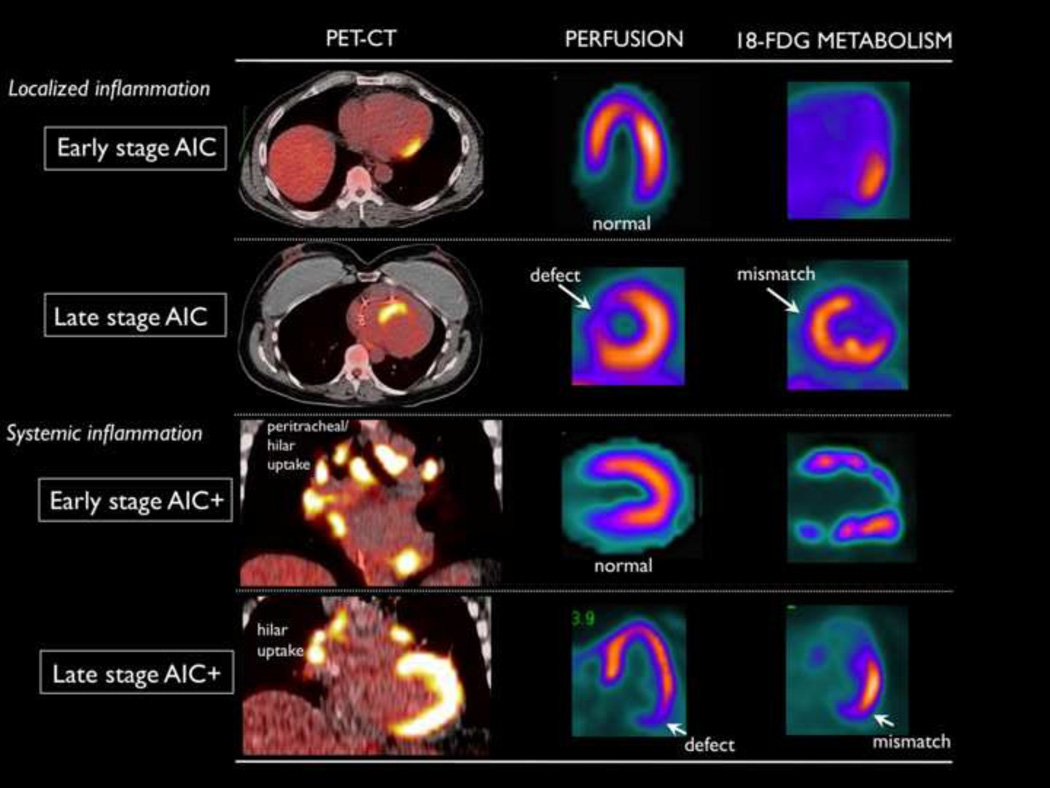
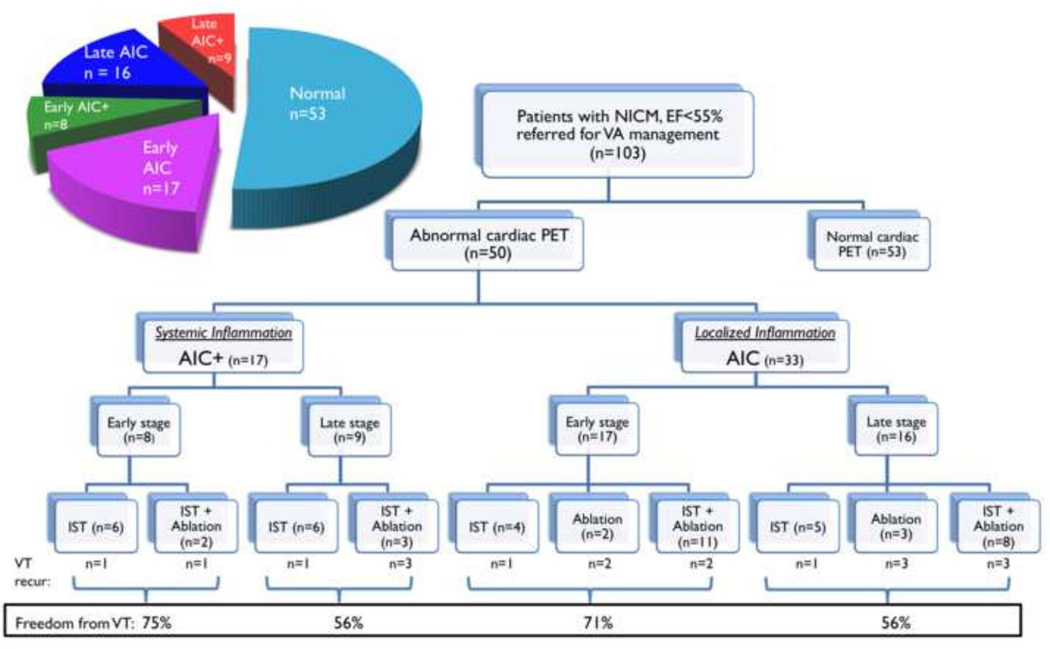
Methods: Fluorine-18 fluoro-2-deoxyglucose (18-FDG) PET/computed tomographic (CT) scans with a >16-hour fasting protocol were prospectively ordered for patients referred for VA and unexplained cardiomyopathy (ejection fraction <55%). Patients with focal myocardial FDG uptake were labeled as arrhythmogenic inflammatory cardiomyopathy (AIC) and classified into 4 groups based on the presence of lymph node uptake (AIC+) and perfusion abnormalities (early vs late stage).
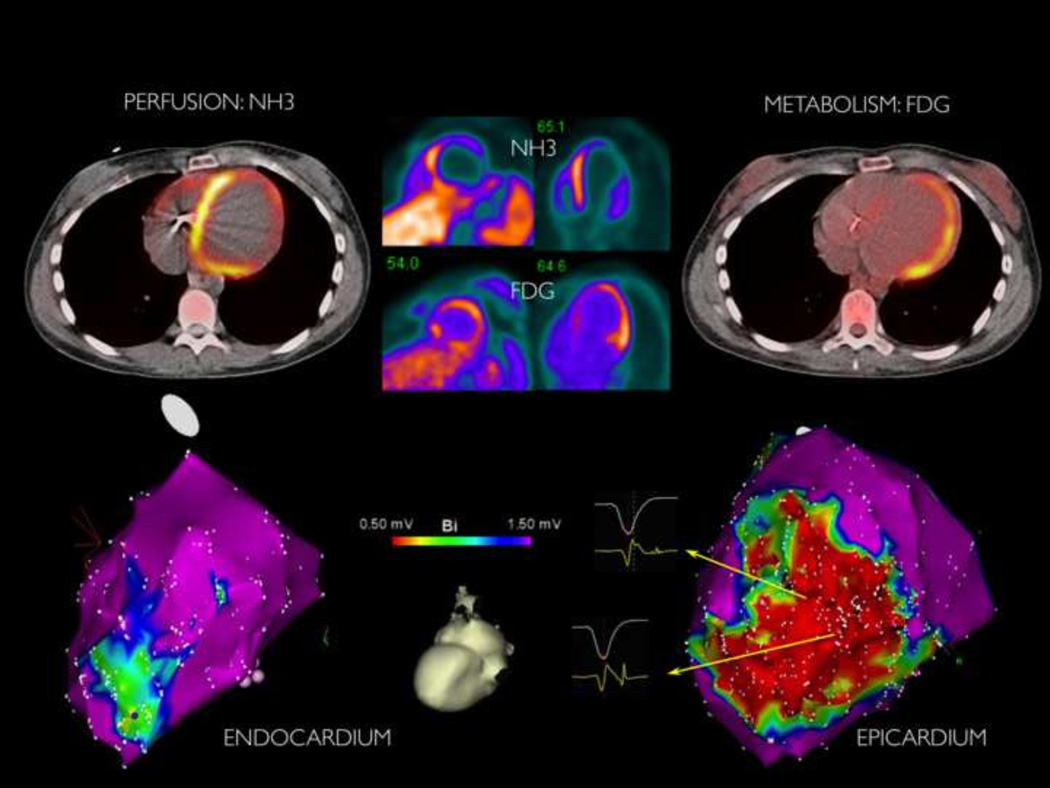
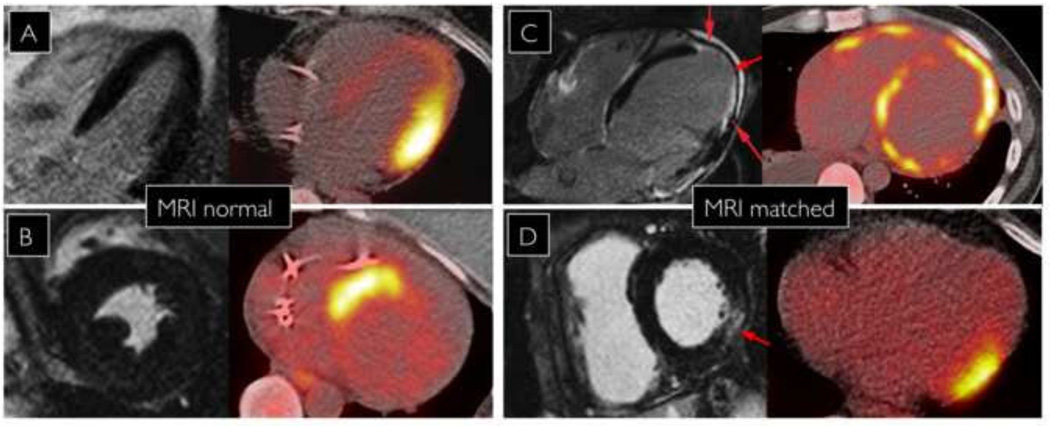
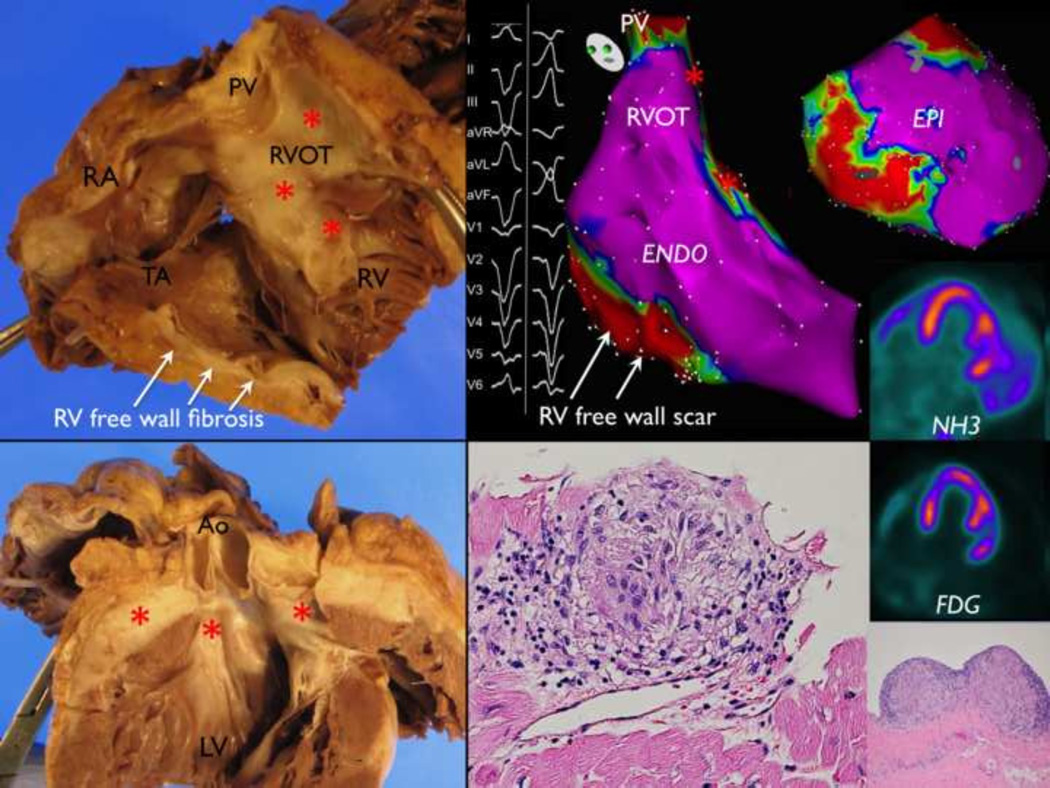
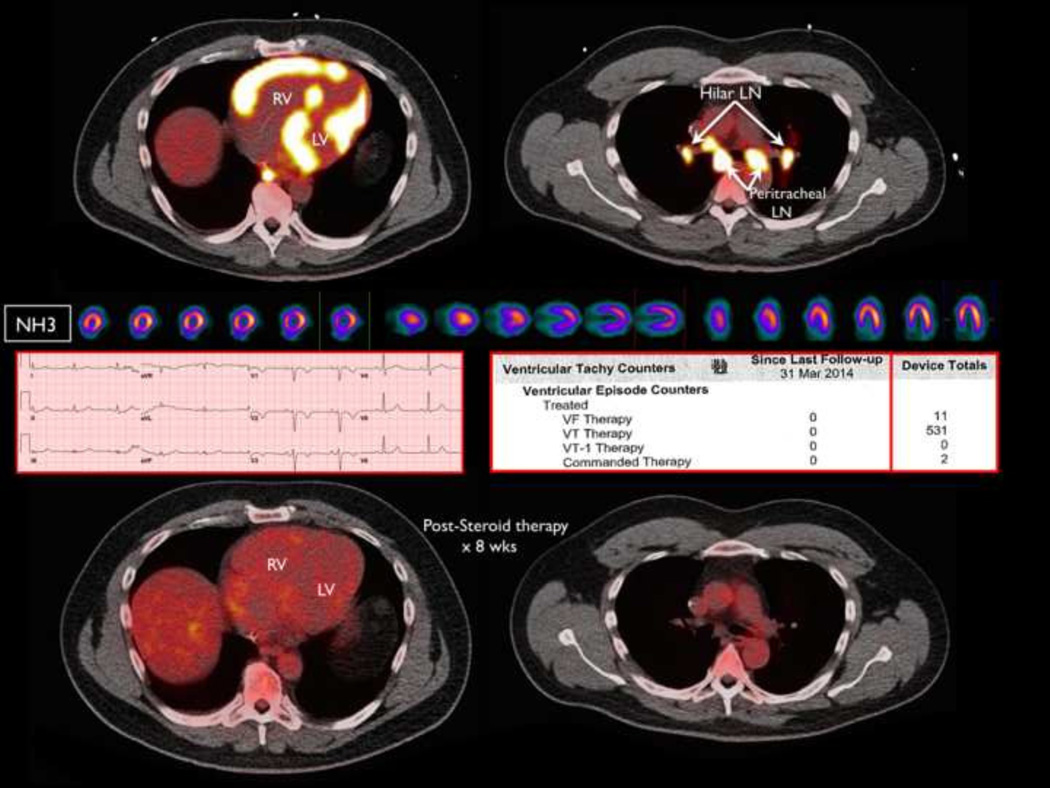
Results: Over a 3-year period, 103 PET scans were performed, with 49% (AIC+ 17, AIC 33) exhibiting focal FDG uptake. Mean patient age was 52 ± 12 years (ejection fraction 36% ± 16%). Patients with AIC were more likely to have a history of pacemaker (32% vs 6%, P = .002) compared to those with normal PET. When biopsy was performed, histologic diagnosis revealed nongranulomatous inflammation in 6 patients and sarcoidosis in 18 patients. Ninety percent of patients with AIC/AIC+ were prescribed immunosuppressive therapy, and 58% underwent ablation. Correlation between low voltage regions on electroanatomic mapping and FDG uptake was observed in 74%. Magnetic resonance imaging findings matched abnormal PET regions in only 40%.
Conclusion: Nearly 50% of patients referred with unexplained cardiomyopathy and VA demonstrate ongoing focal myocardial inflammation on FDG PET. These data suggest that a significant proportion of patients labeled "idiopathic" may have occult AIC, which may benefit from early detection and immunosuppressive medical therapy.
Keywords: Cardiomyopathy; Inflammation; Positron emission tomography; Ventricular arrhythmia.
Published by Elsevier Inc.
Conflict of interest statement
Conflicts of Interest: None
Figures
References
-
- Sacher F, Tedrow UB, Field ME, Raymond JM, Koplan BA, Epstein LM, Stevenson WG. Ventricular tachycardia ablation: evolution of patients and procedures over 8 years. Circ Arrhythm Electrophysiol. 2008;1:153–161. - PubMed
-
- Kindermann I, Barth C, Mahfoud F, Ukena C, Lenski M, Yilmaz A, Klingel K, Kandolf R, Sechtem U, Cooper LT, Bohm M. Update on myocarditis. J Am Coll Cardiol. 2012;59:779–792. - PubMed
-
- Koplan BA, Soejima K, Baughman K, Epstein LM, Stevenson WG. Refractory ventricular tachycardia secondary to cardiac sarcoid: electrophysiologic characteristics, mapping, and ablation. Heart Rhythm. 2006;3:924–929. - PubMed
-
- Thachil A, Christopher J, Sastry BK, Reddy KN, Tourani VK, Hassan A, Raju BS, Narasimhan C. Monomorphic ventricular tachycardia and mediastinal adenopathy due to granulomatous infiltration in patients with preserved ventricular function. J Am Coll Cardiol. 2011;58:48–55. - PubMed
-
- Ishimaru S, Tsujino I, Takei T, Tsukamoto E, Sakaue S, Kamigaki M, Ito N, Ohira H, Ikeda D, Tamaki N, Nishimura M. Focal uptake on 18F-fluoro-2-deoxyglucose positron emission tomography images indicates cardiac involvement of sarcoidosis. Eur Heart J. 2005;26:1538–1543. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
