

Personalized Immunomodulatory Therapy for Atopic Dermatitis: An Allergist's View
- PMID: 26273148
- PMCID: PMC4530142
- DOI: 10.5021/ad.2015.27.4.355
Personalized Immunomodulatory Therapy for Atopic Dermatitis: An Allergist's View
Abstract
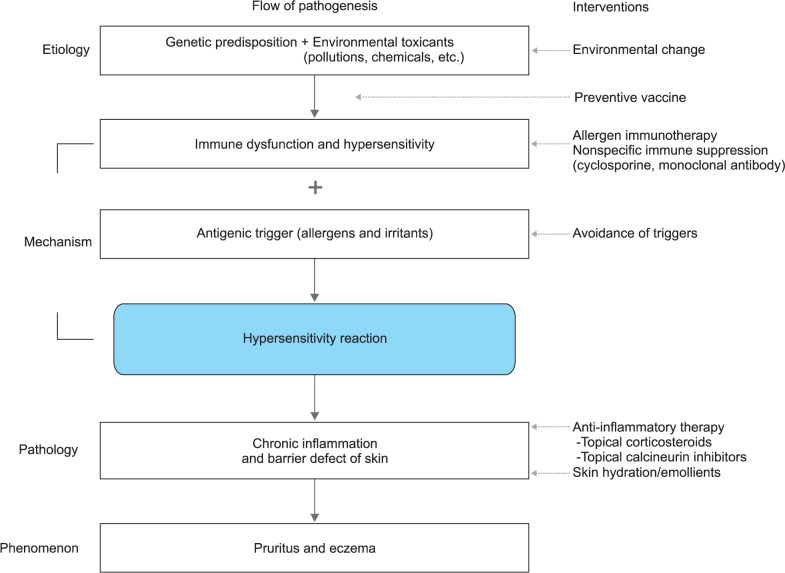
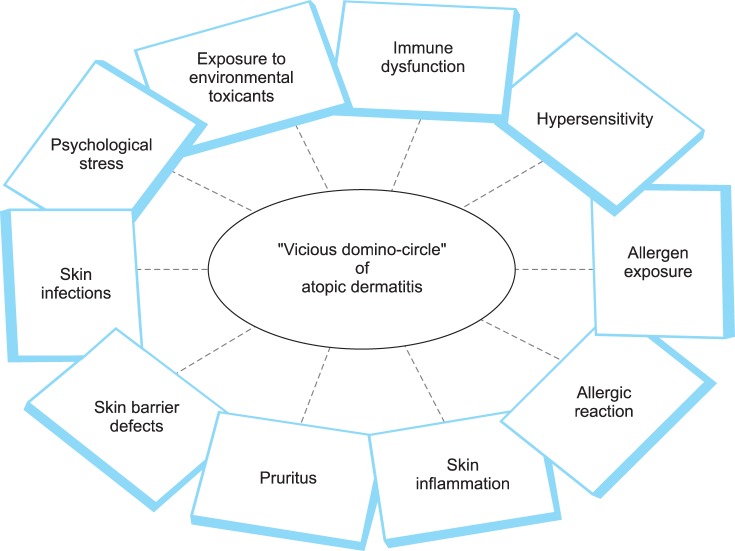
The current standard medical therapy for atopic dermatitis (AD) mainly focuses on symptomatic relief by controlling skin inflammation with topical corticosteroids and/or topical calcineurin inhibitors. However, the clinical efficacy of pharmacological therapy is often disappointing to both patients and physicians. The terminology of AD contains a historical meaning of eczematous dermatitis caused by hypersensitivity reaction to environmental inhalant or food allergen. Complex interrelationships among genetic abnormalities, environmental triggers, skin barrier defects, and immune dysfunction resulting in a vicious domino-circle seem to be involved in the development and maintenance of AD. In the viewpoint of AD as an allergic disease, complete avoidance of clinically relevant allergen or induction of specific immune tolerance through administrations of allergen (allergen immunotherapy) can provide clinical remission by breaking the vicious domino-circle maintaining a chronic disease state. In recent clinical studies, monoclonal antibodies including the anti-interleukin-4 receptor antibody and anti-B cell antibody induced significant clinical improvements in patients with AD. The detailed characteristics of immune dysfunction are heterogeneous among patients with AD. Therefore, a personalized combination of immunomodulatory therapies to reduce hypersensitivity (allergen immunotherapy) and correct immune dysfunction (monoclonal antibody therapy) could be a reasonable therapeutic approach for patients with AD. Future immunomodulatory therapies for AD should be developed to achieve long-term treatment-free clinical remission by induction of immune tolerance.
Keywords: Allergens; Atopic dermatitis; Hypersensitivity; Immunomodulation; Therapeutics.
Figures
Similar articles
-
Regulatory T Cell-Targeted Immunomodulatory Therapy for Long-Term Clinical Improvement of Atopic Dermatitis: Hypotheses and Perspectives.Life (Basel). 2023 Aug 1;13(8):1674. doi: 10.3390/life13081674. Life (Basel). 2023. PMID: 37629531 Free PMC article. Review.
-
Allergic manifestations of skin diseases--atopic dermatitis.Chem Immunol Allergy. 2006;91:76-86. doi: 10.1159/000090231. Chem Immunol Allergy. 2006. PMID: 16354950 Review.
-
IgE-mediated hypersensitivity and contact sensitivity to multiple environmental allergens in atopic dermatitis.Arch Dermatol. 1994 Nov;130(11):1393-401. Arch Dermatol. 1994. PMID: 7979440
-
Non-pharmacological therapies and their efficacy in atopic dermatitis: A narrative review.Indian J Dermatol Venereol Leprol. 2025 Apr 24:1-9. doi: 10.25259/IJDVL_1076_2024. Online ahead of print. Indian J Dermatol Venereol Leprol. 2025. PMID: 40357939 Review.
-
Long-term management of moderate-to-severe atopic dermatitis with dupilumab and concomitant topical corticosteroids (LIBERTY AD CHRONOS): a 1-year, randomised, double-blinded, placebo-controlled, phase 3 trial.Lancet. 2017 Jun 10;389(10086):2287-2303. doi: 10.1016/S0140-6736(17)31191-1. Epub 2017 May 4. Lancet. 2017. PMID: 28478972 Clinical Trial.
Cited by
-
Autologous Immunoglobulin Therapy in Patients With Severe Recalcitrant Atopic Dermatitis: Long-Term Changes of Clinical Severity and Laboratory Parameters.Allergy Asthma Immunol Res. 2016 Jul;8(4):375-82. doi: 10.4168/aair.2016.8.4.375. Allergy Asthma Immunol Res. 2016. PMID: 27126731 Free PMC article.
-
Regulatory T Cell-Targeted Immunomodulatory Therapy for Long-Term Clinical Improvement of Atopic Dermatitis: Hypotheses and Perspectives.Life (Basel). 2023 Aug 1;13(8):1674. doi: 10.3390/life13081674. Life (Basel). 2023. PMID: 37629531 Free PMC article. Review.
-
Associations of Atopic Dermatitis With Obesity and Unmarried Status in Young Adults: Evidence for Atopic Dermatitis as a Life-Style Disorder With High Social Impact.Allergy Asthma Immunol Res. 2016 Mar;8(2):89-91. doi: 10.4168/aair.2016.8.2.89. Allergy Asthma Immunol Res. 2016. PMID: 26739400 Free PMC article. No abstract available.
-
Psoriasis and Atopic Dermatitis.Dermatol Ther (Heidelb). 2017 Jan;7(Suppl 1):31-41. doi: 10.1007/s13555-016-0167-9. Epub 2017 Feb 1. Dermatol Ther (Heidelb). 2017. PMID: 28150106 Free PMC article. Review.
-
Intramuscular Injection of Autologous Serum in Adolescent and Adult Patients with Atopic Dermatitis: A Preliminary Randomized Clinical Trial.Yonsei Med J. 2023 Jul;64(7):423-432. doi: 10.3349/ymj.2022.0559. Yonsei Med J. 2023. PMID: 37365736 Free PMC article. Clinical Trial.
References
-
- Akdis CA, Akdis M, Bieber T, Bindslev-Jensen C, Boguniewicz M, Eigenmann P, et al. European Academy of Allergology and Clinical Immunology/American Academy of Allergy, Asthma and Immunology. Diagnosis and treatment of atopic dermatitis in children and adults: European Academy of Allergology and Clinical Immunology/American Academy of Allergy, Asthma and Immunology/PRACTALL Consensus Report. J Allergy Clin Immunol. 2006;118:152–169. - PubMed
-
- Novak N, Bieber T, Leung DY. Immune mechanisms leading to atopic dermatitis. J Allergy Clin Immunol. 2003;112(6 Suppl):S128–S139. - PubMed
-
- Beck LA, Thaçi D, Hamilton JD, Graham NM, Bieber T, Rocklin R, et al. Dupilumab treatment in adults with moderate-to-severe atopic dermatitis. N Engl J Med. 2014;371:130–139. - PubMed
-
- Simon D, Hösli S, Kostylina G, Yawalkar N, Simon HU. Anti-CD20 (rituximab) treatment improves atopic eczema. J Allergy Clin Immunol. 2008;121:122–128. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
