

Development of a novel radiographic measure of lumbar instability and validation using the facet fluid sign
- PMID: 26273555
- PMCID: PMC4528437
- DOI: 10.14444/2037
Development of a novel radiographic measure of lumbar instability and validation using the facet fluid sign
Abstract
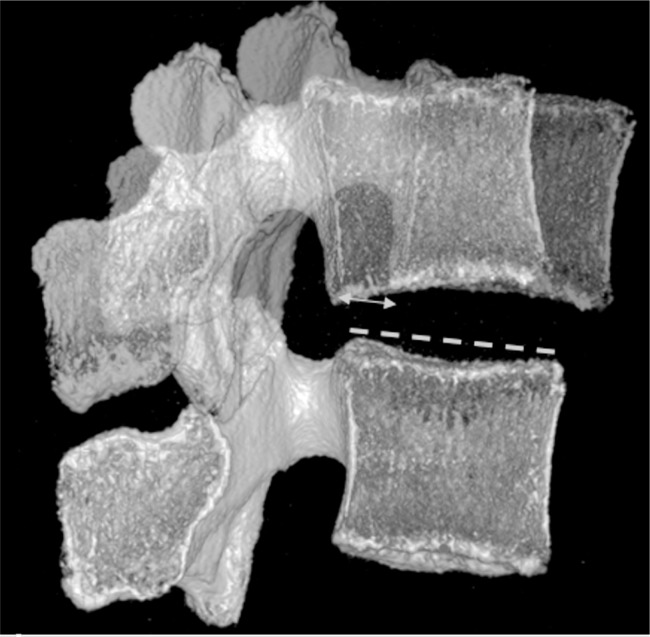
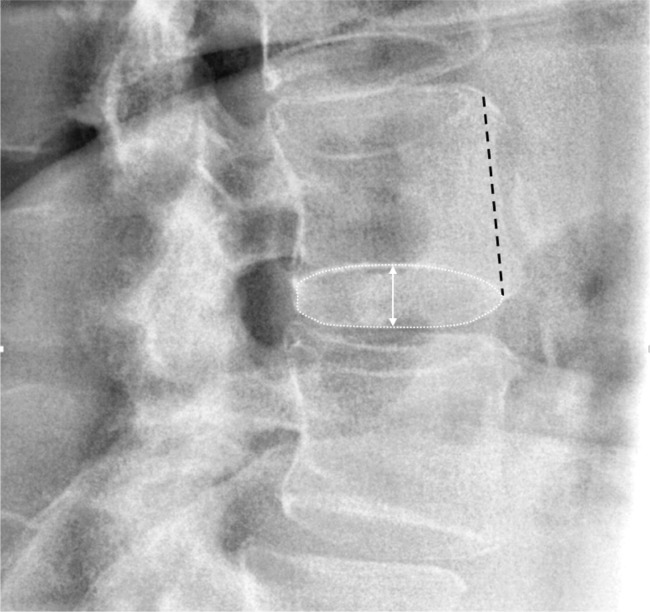
Background: Lumbar spinal instability is frequently referenced in clinical practice and the scientific literature despite the lack of a standard definition or validated radiographic test. The Quantitative Stability Index (QSI) is being developed as a novel objective test for sagittal plane lumbar instability. The QSI is calculated using lumbar flexion-extension radiographs. The goal of the current study was to use the facet fluid sign on MRI as the "gold standard" and determine if the QSI is significantly different in the presence of the fluid sign.
Methods: Sixty-two paired preoperative MRI and flexion-extension exams were obtained from a large FDA IDE study. The MRI exams were assessed for the presence of a facet fluid sign, and the QSI was calculated from sagittal plane intervertebral rotation and translation measurements. The QSI is based on the translation per degree of rotation (TPDR) and is calculated as a Z-score. A QSI > 2 indicates that the TPDR is > 2 std dev above the mean for an asymptomatic and radiographically normal population. The reproducibility of the QSI was also tested.
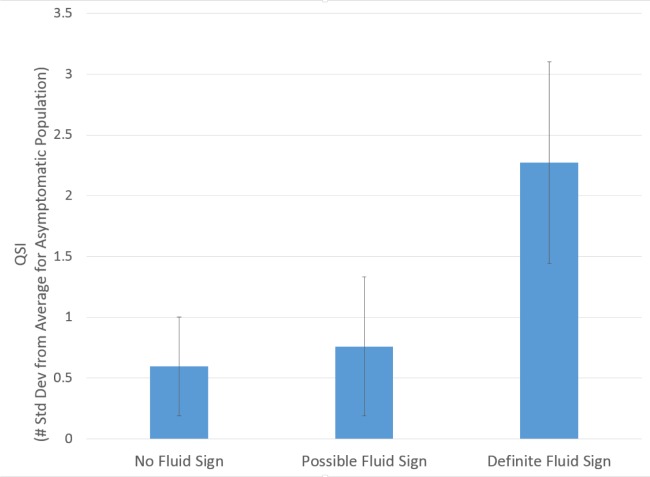
Results: The mean difference between trained observers in the measured QSI was between -0.28 and 0.36. The average QSI was significantly (P = 0.047, one-way analysis of variance) higher at levels with a definite fluid sign (2.3±3.2 versus 0.60±2.4).
Conclusions: Although imperfect, the facet fluid sign observed may be the best currently available test for lumbar spine instability. Using the facet fluid sign as the "gold standard" the current study documents that the QSI can be expected to be significantly higher in the presence of the facet fluid sign. This supports that QSI might be used to test for sagittal plane lumbar instability.
Clinical relevance: A validated, objective and practical test for spinal instability would facilitate research to understand the importance of instability in diagnosis and treatment of low-back related disorders.
Keywords: Instability; QSI; fluid sign; lumbar spine; radiographic.
Figures
References
-
- Morgan FP, King T. Primary instability of lumbar vertebrae as a common cause of low back pain. J Bone Joint Surg Br. 1957;39-B(1):6–22. - PubMed
-
- Knutsson F. The instability associated with disc degeneration in the lumbar spine. Acta Radiol. 1944;25:593–8.
-
- Weiler PJ, King GJ, Gertzbein SD. Analysis of sagittal plane instability of the lumbar spine in vivo. Spine. 1990;15(12):1300–6. - PubMed
-
- Hasegawa K, Kitahara K, Shimoda H, Hara T. Facet joint opening in lumbar degenerative diseases indicating segmental instability. J Neurosurg: Spine. 2010;12(6):687–93. - PubMed
-
- Rihn JA, Lee JY, Khan M, Ulibarri JA, Tannoury C, Donaldson WF, III, et al. Does lumbar facet fluid detected on magnetic resonance imaging correlate with radiographic instability in patients with degenerative lumbar disease? Spine. 2007;32(14):1555–60. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials