

Management of adult spontaneous spondylodiscitis and its rising incidence
- PMID: 26274746
- PMCID: PMC5126242
- DOI: 10.1308/rcsann.2015.0009
Management of adult spontaneous spondylodiscitis and its rising incidence
Abstract
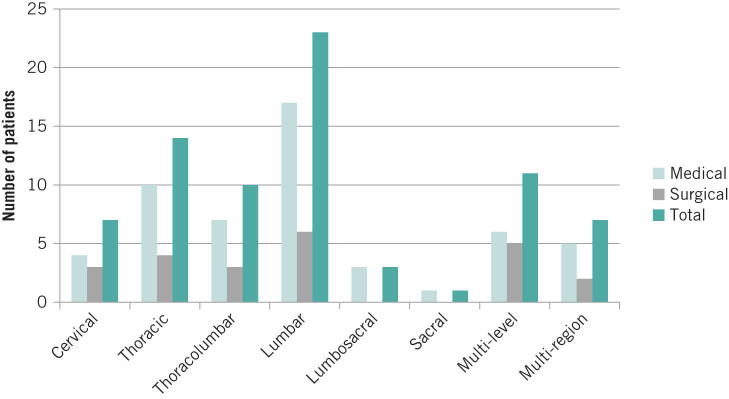
Introduction: Spondylodiscitis refers to the infection of the intervertebral disc and osteomyelitis of the adjacent endplates, and it is uncommon in the developed world. Broad consensus indicates its incidence is on the rise.
Methods: The aim of this retrospective study was twofold. First, we sought to give an up-to-date incidence estimate by comparing case presentation over two time periods (1995-1999 and 2008-2011). Data from the England and Wales census in 2001 and 2011 were used for incidence estimation. The second part of this study aimed to generate management guidance from data from medical and radiographic records of the 2008-2011 patient cohort.
Results: The incidence of adult spontaneous spondylodiscitis in the local region between 2008 and 2011 was 3.67/100,000 per year, representing a 150% increase from the incidence in 1995-1999. Our data demonstrate that methicillin sensitive Staphylococcus aureus remains the most common offending pathogen of spontaneous spondylodiscitis. The mean C-reactive protein (CRP) level remained at >30mg/l after a month of starting antibiotic treatment in both medically and surgically managed groups.
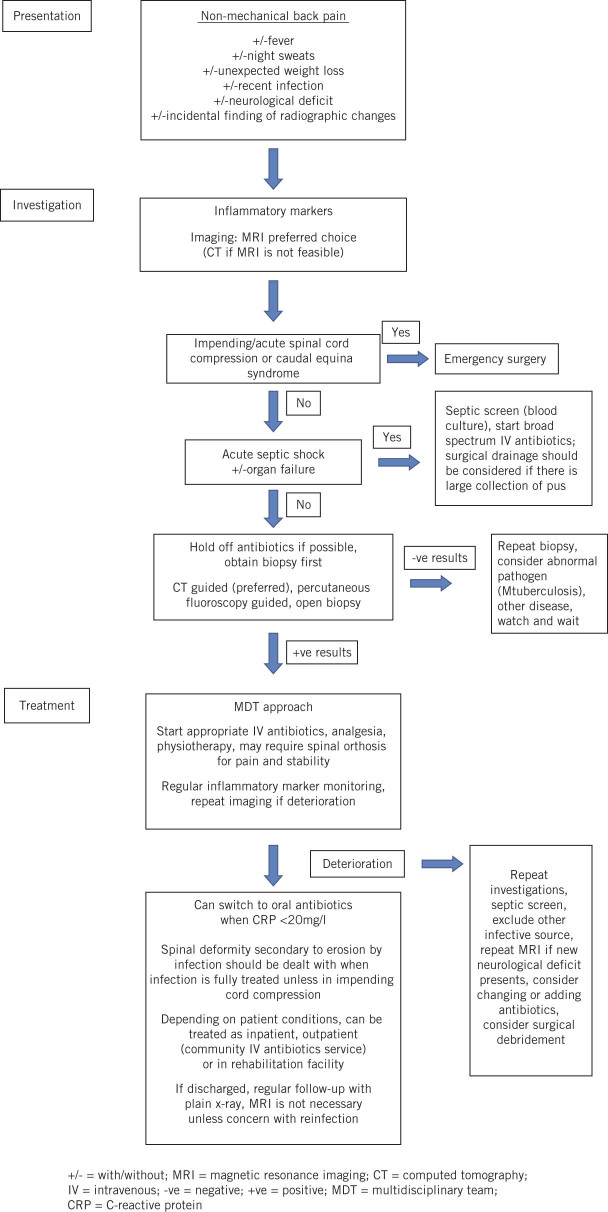
Conclusions: Evidence suggests that the incidence of spondylodiscitis is on the rise. A review of our case series has demonstrated the effectiveness of intravenous antibiotic therapy. While no official guidance exists for when to switch from intravenous to oral antibiotics, our study shows that CRP at 1 month is >30mg/l and we recommend 6 weeks of intravenous therapy, followed by 6 further weeks of oral therapy.
Keywords: Antibiotic; Discitis; Disease management; Incidence.
Figures
References
-
- Cottle L, Riordan T. Infectious spondylodiscitis. J Infect 2008; : 401–412. - PubMed
-
- Skaf GS, Domloj NT, Fehlings MG, et al. . Pyogenic spondylodiscitis: an overview. J Infect Public Health 2010; : 5–16. - PubMed
-
- Carragee EJ. Pyogenic vertebral osteomyelitis. J Bone Joint Surg Am 1997; : 874–880. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous