

Counselling versus low-intensity cognitive behavioural therapy for persistent sub-threshold and mild depression (CLICD): a pilot/feasibility randomised controlled trial
- PMID: 26275718
- PMCID: PMC4536887
- DOI: 10.1186/s12888-015-0582-y
Counselling versus low-intensity cognitive behavioural therapy for persistent sub-threshold and mild depression (CLICD): a pilot/feasibility randomised controlled trial
Abstract
Background: Persistent depressive symptoms below the threshold criteria for major depression represent a chronic condition with high risk of progression to a diagnosis of major depression. The evidence base for psychological treatments such as Person-Centred Counselling and Low-Intensity Cognitive Behavioural Therapy for sub-threshold depressive symptoms and mild depression is limited, particularly for longer-term outcomes.
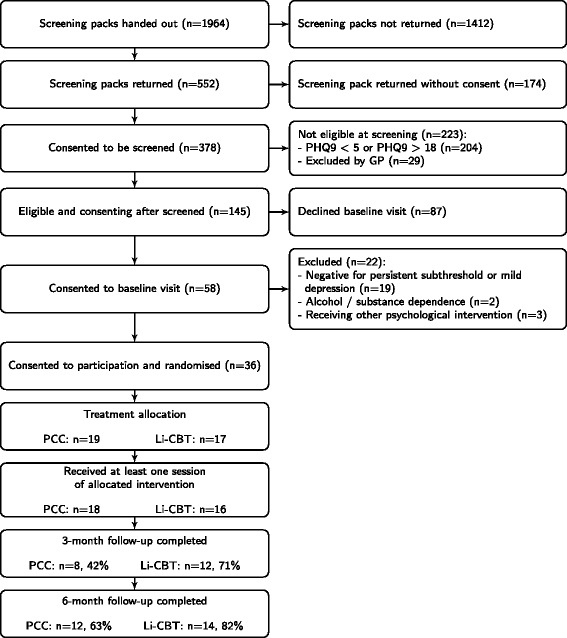
Methods: This study aimed to test the feasibility of delivering a randomised controlled trial into the clinical and cost effectiveness of Low-Intensity Cognitive Behavioural Therapy versus Person-Centred Counselling for patients with persistent sub-threshold depressive symptoms and mild depression. The primary outcome measures for this pilot/feasibility trial were recruitment, adherence and retention rates at six months from baseline. An important secondary outcome measure was recovery from, or prevention of, depression at six months assessed via a structured clinical interview by an independent assessor blind to the participant's treatment condition. Thirty-six patients were recruited in five general practices and were randomised to either eight weekly sessions of person-centred counselling each lasting up to an hour, or up to eight weeks of cognitive-behavioural self-help resources with guided telephone support sessions lasting 20-30 minutes each.
Results: Recruitment rate in relation to the number of patients approached at the general practices was 1.8 %. Patients attended an average of 5.5 sessions in both interventions. Retention rate for the 6-month follow-up assessments was 72.2 %. Of participants assessed at six months, 71.4 % of participants with a diagnosis of mild depression at baseline had recovered, while 66.7 % with a diagnosis of persistent subthreshold depression at baseline had not developed major depression. There were no significant differences between treatment groups for both recovery and prevention of depression at six months or on any of the outcome measures.
Conclusions: It is feasible to recruit participants and successfully deliver both interventions in a primary care setting to patients with subthreshold and mild depression; however recruiting requires significant input at the general practices. The evidence from this study suggests that short-term Person-Centred Counselling and Low-Intensity Cognitive Behaviour Therapy are potentially effective and their effectiveness should be evaluated in a larger randomised controlled study which includes a health economic evaluation.
Trial registration: Current Controlled Trials ISRCTN60972025 .
Figures
Similar articles
-
Counselling versus Low-Intensity Cognitive Behavioural Therapy for persistent sub-threshold and mild Depression (CLICD): study protocol for a pilot/feasibility randomised controlled trial.Springerplus. 2014 Nov 5;3:654. doi: 10.1186/2193-1801-3-654. eCollection 2014. Springerplus. 2014. PMID: 25392813 Free PMC article.
-
Randomised controlled trial of non-directive counselling, cognitive-behaviour therapy and usual general practitioner care in the management of depression as well as mixed anxiety and depression in primary care.Health Technol Assess. 2000;4(19):1-83. Health Technol Assess. 2000. PMID: 11086269 Clinical Trial.
-
Guided, internet-based, rumination-focused cognitive behavioural therapy (i-RFCBT) versus a no-intervention control to prevent depression in high-ruminating young adults, along with an adjunct assessment of the feasibility of unguided i-RFCBT, in the REducing Stress and Preventing Depression trial (RESPOND): study protocol for a phase III randomised controlled trial.Trials. 2016 Jan 4;17:1. doi: 10.1186/s13063-015-1128-9. Trials. 2016. PMID: 26725476 Free PMC article. Clinical Trial.
-
Novel Augmentation Strategies in Major Depression.Dan Med J. 2017 Apr;64(4):B5338. Dan Med J. 2017. PMID: 28385173 Review.
-
Effectiveness of client-centred counselling on weight management among Black African women with overweight and obesity in high-income countries: a systematic review.Psychol Health. 2025 Mar 11:1-32. doi: 10.1080/08870446.2025.2475161. Online ahead of print. Psychol Health. 2025. PMID: 40066757 Review.
Cited by
-
A pragmatic randomised controlled trial assessing the non-inferiority of counselling for depression versus cognitive-behaviour therapy for patients in primary care meeting a diagnosis of moderate or severe depression (PRaCTICED): Study protocol for a randomised controlled trial.Trials. 2017 Mar 1;18(1):93. doi: 10.1186/s13063-017-1834-6. Trials. 2017. PMID: 28249592 Free PMC article. Clinical Trial.
-
Effectiveness of Dance Movement Therapy in the Treatment of Adults With Depression: A Systematic Review With Meta-Analyses.Front Psychol. 2019 May 3;10:936. doi: 10.3389/fpsyg.2019.00936. eCollection 2019. Front Psychol. 2019. PMID: 31130889 Free PMC article.
-
A brief, multidimensional measure of clients' therapy preferences: The Cooper-Norcross Inventory of Preferences (C-NIP).Int J Clin Health Psychol. 2016 Jan-Apr;16(1):87-98. doi: 10.1016/j.ijchp.2015.08.003. Epub 2015 Sep 18. Int J Clin Health Psychol. 2016. PMID: 30487853 Free PMC article.
-
Who is seeking whom? A person-centred approach to help-seeking in adults with currently untreated mental health problems via latent class analysis.Soc Psychiatry Psychiatr Epidemiol. 2018 Aug;53(8):773-783. doi: 10.1007/s00127-018-1537-7. Epub 2018 Jun 6. Soc Psychiatry Psychiatr Epidemiol. 2018. PMID: 29876581
-
Minor depression in older, long-term unemployed people seeking vocational support.BMC Psychiatry. 2017 Jul 5;17(1):243. doi: 10.1186/s12888-017-1404-1. BMC Psychiatry. 2017. PMID: 28679439 Free PMC article.
References
-
- Goldberg D, Huxley P. Common mental disorders: a bio-social model. London: Routledge; 1992.
-
- National Institute for Health and Care Excellence. Clinical Guideline 90, Depression in adults: The treatment and management of depression in adults. London: National Institute for Health and Care Excellence; 2009. https://www.nice.org.uk/guidance/cg90. Accessed 21 April 2015.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
