

Antimalarial drugs for preventing malaria during pregnancy and the risk of low birth weight: a systematic review and meta-analysis of randomized and quasi-randomized trials
- PMID: 26275820
- PMCID: PMC4537579
- DOI: 10.1186/s12916-015-0429-x
Antimalarial drugs for preventing malaria during pregnancy and the risk of low birth weight: a systematic review and meta-analysis of randomized and quasi-randomized trials
Abstract
Background: It is known that antimalarial drugs reduce the risk of low birth weight (LBW) in pregnant patients. However, a previous Cochrane review did not evaluate whether the level of antimalarial drug resistance could modify the protective effect of antimalarial drugs in this regard. In addition, no systematic review exists comparing current recommendations for malaria prevention during pregnancy to alternative regimens in Africa. Therefore, we conducted a comprehensive systematic review and meta-analysis to assess the efficacy of antimalarial drugs for malaria prevention during pregnancy in reducing the risk of LBW.
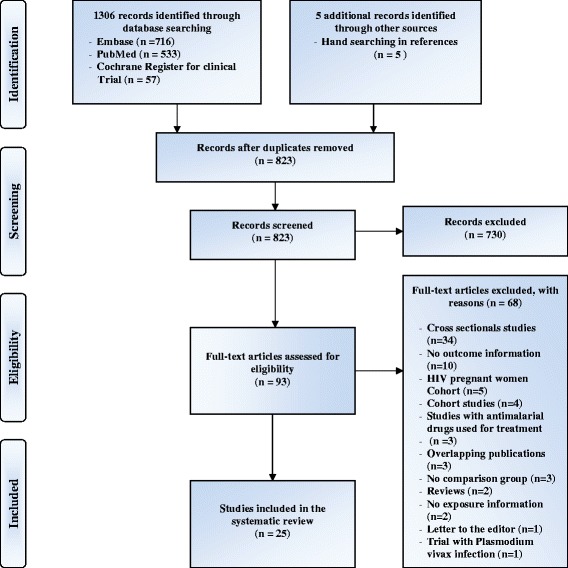
Methods: We searched PubMed, Embase and the Cochrane Central Register of Controlled Trials (CENTRAL) for articles published up to 21 November 2014, in English or French, and identified additional studies from reference lists. We included randomized and quasi-randomized studies reporting LBW as one of the outcomes. We extracted data and assessed the risk of bias in selected studies. All pooled analyses were based on a random effect model, and we used a funnel plot and trim and fill method to test and adjust for publication bias.
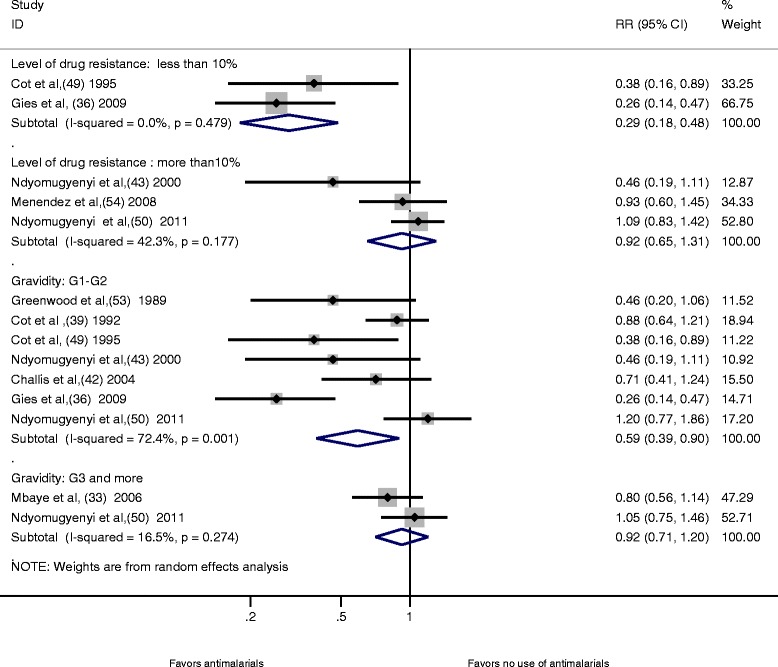
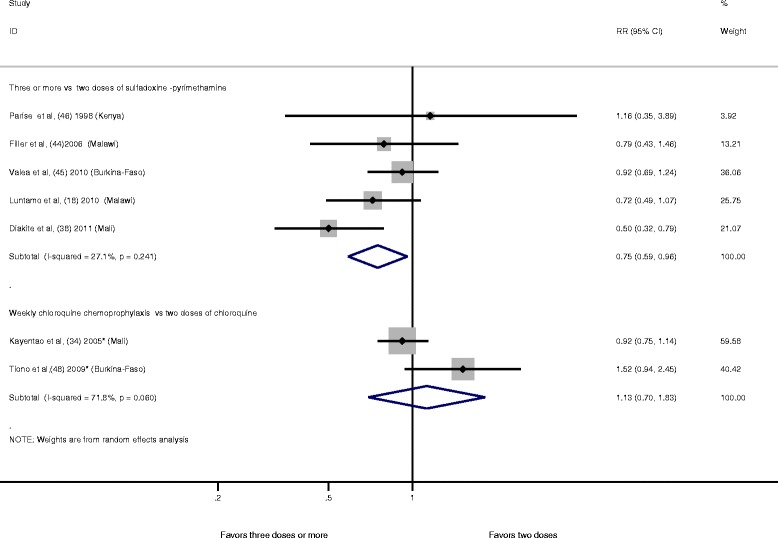
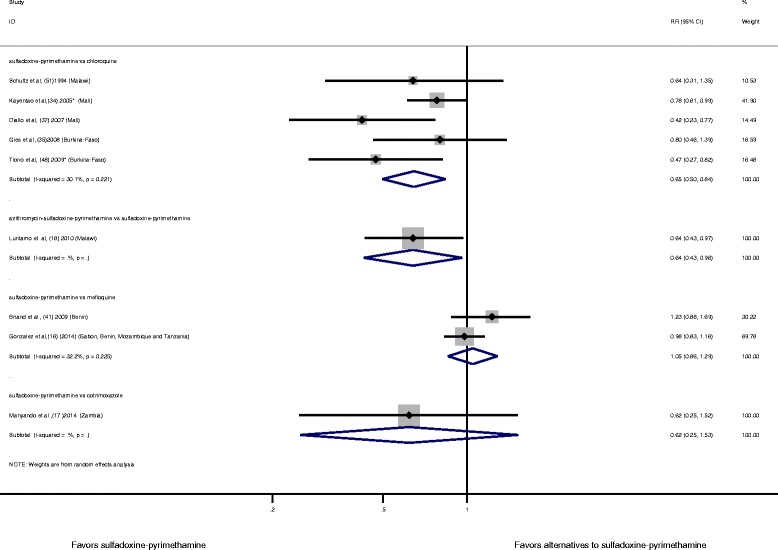
Results: A total of 25 studies met the inclusion criteria (37,981 subjects). Compared to no use, all combined antimalarial drugs were associated with a 27% (RR 0.73, 95% CI 0.56-0.97, ten studies) reduction in the risk of LBW. The level of antimalarial drug resistance modified the protective effect of the antimalarial drug used for prevention of LBW during pregnancy. Sulfadoxine-pyrimethamine was not associated with a reduction in the risk of LBW in regions where the prevalence of the dihydropteroate synthase 540E mutation exceeds 50% (RR 0.99, 95% CI 0.80-1.22, three studies). The risk of LBW was similar when sulfadoxine-pyrimethamine was compared to mefloquine (RR 1.05, 95% CI 0.86-1.29, two studies).
Conclusion: Prophylactic antimalarial drugs and specifically sulfadoxine-pyrimethamine may no longer protect against the risk of LBW in areas of high-level resistance. In Africa, there are currently no suitable alternative drugs to replace sulfadoxine-pyrimethamine for malaria prevention during pregnancy.
Figures

References
-
- Wagstaff A, Claeson M, Hecht RM, Gottret P, Fang Q, et al. Millennium Development Goals for health: what will it take to accelerate progress? In: Jamison DT, Breman JG, Measham AR, Alleyne G, Claeson M, Evans DB, et al., editors. Disease control priorities in developing countries. 2. Washington, DC: The International Bank for Reconstruction and Development/The World Bank Group; 2006. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
